 Article
in Press Printer-friendly PDF file
Article
in Press Printer-friendly PDF fileWestside Observer Newspaper
April 2016 at www.WestsideObserver.com
LHH’s “Mission Statement” Changed, Again!
Skilled Nursing Bed Shortage Worsens
Article
in Press Printer-friendly PDF file
Westside Observer Newspaper
April 2016 at www.WestsideObserver.com
LHH’s
“Mission Statement” Changed, Again!
Skilled Nursing
Bed Shortage Worsens
by Patrick Monette-Shaw
How can San Francisco officials say with a straight face that there are no beds at the inn for elderly and disabled San Franciscans, saying there are not enough skilled nursing facility (SNF), board and care, and post-acute care beds, after decades of planning?
After all, these public officials were charged with planning for these various levels of care. What happened to their grand plans?
A new report from the Department of Public Health — “Framing San Francisco’s Post-Acute Care Shortage” — belatedly calls for yet more planning, since previous planning has been anything but meaningful.
I have covered the loss of skilled nursing beds in San Francisco — and the utter lack of planning for SNF level of care — in a series of articles over the past seven years, including “Laguna Honda Hospital: Pot-bellies vs. Beds” (July 2009), “Who’s Dumping Grandma?” (June 2013), “The Big Squeeze: Dys-Integration of ’Old Friends’ ” (July 2014), and “Detrimental Skilled Nursing Cuts” (June 2015). Other articles I’ve written going back to 2004 also touched on the loss of SNF beds.
 Despite previous
reporting on the crisis, the situation has clearly grown worse
over the past seven years, since we now learn that San Francisco
appears to be facing a 1,745-bed SNF shortage 14 years from now
in 2030.
Despite previous
reporting on the crisis, the situation has clearly grown worse
over the past seven years, since we now learn that San Francisco
appears to be facing a 1,745-bed SNF shortage 14 years from now
in 2030.
How did San Francisco get to this point?
Framing the Skilled Nursing Bed Challenge
Rather than honestly reporting that the main problem is a lack of skilled nursing beds in San Francisco, a new report represented to the Health Commission on February 16 — “Framing San Francisco’s Post-Acute Care Shortage” — is too little, too late, and entirely predictable.
 Instead of admitting
in the report’s title that there is a “skilled
nursing bed” shortage, the City is trying to re-frame
and misdirect the discussion — for the benefit of private-sector
hospital “partners” — that there is a “post-acute
care bed” shortage, that has principally been the
private-sector hospital’s own fault since they have been
shedding in-house post-acute care beds, and eliminating hospital-based
SNF beds, for now decades.
Instead of admitting
in the report’s title that there is a “skilled
nursing bed” shortage, the City is trying to re-frame
and misdirect the discussion — for the benefit of private-sector
hospital “partners” — that there is a “post-acute
care bed” shortage, that has principally been the
private-sector hospital’s own fault since they have been
shedding in-house post-acute care beds, and eliminating hospital-based
SNF beds, for now decades.
The distinction between the two levels of care may not be just mere semantics.
According to Wikipedia, “Acute care” is “a branch of secondary healthcare where a patient receives active but short-term treatment for a severe injury or episode of illness, for an urgent medical condition, or during recovery from surgery. In medical terms, care for acute health conditions is the opposite from chronic care,” or “long-term care,” or preventive care.
Alternatively, subacute care is defined as skilled nursing beds for patients who don’t require care in an acute hospital, but require more intensive skilled nursing care than is typically provided to the majority of patients in a SNF. Subacute patients are typically medically fragile, and require specialized nursing services such as tracheotomy care, IV tube feeding, complex wound management, or inhalation therapy. St. Luke’s is the only hospital still providing sub-acute level of care in San Francisco and those beds are also on the chopping block, too — apparently to be eliminated by 2019.
 Private-sector hospitals
have been shutting down their in-house sub-acute, post-acute,
and SNF beds for well over a decade, claiming they are too expensive
to operate, and appear to be foisting the need for such beds onto
the public sector.
Private-sector hospitals
have been shutting down their in-house sub-acute, post-acute,
and SNF beds for well over a decade, claiming they are too expensive
to operate, and appear to be foisting the need for such beds onto
the public sector.
While “SNF-level,” ”Sub-Acute level,” and “Acute care level” may be legal categories with differing staffing and credentialing requirements, along with various required building construction standards, ”post-acute care” may mean anything and everything after “Acute,” and may be a new fashionable term, rather than a distinct level of care.
Details in the New Report
 Significantly, the
“Post-Acute Care Shortage” report documents San
Francisco has seen a 43.3% decline in the number of hospital-based
SNF beds between 2001 and 2015 alone, from 2,331 beds, to just
1,319, as hospitals — by design — eliminated 1,012 SNF
beds across those 14 years. Fully 420 — 41.5% — of the
lost 1,012 SNF beds occurred at Laguna Hospital alone when they
were eliminated from the LHH replacement project.
Significantly, the
“Post-Acute Care Shortage” report documents San
Francisco has seen a 43.3% decline in the number of hospital-based
SNF beds between 2001 and 2015 alone, from 2,331 beds, to just
1,319, as hospitals — by design — eliminated 1,012 SNF
beds across those 14 years. Fully 420 — 41.5% — of the
lost 1,012 SNF beds occurred at Laguna Hospital alone when they
were eliminated from the LHH replacement project.
[Editor: In April 2015, DPH projected there would be a 42.8% decline of hospital-based SNF beds between 2002 and 2020, but it now appears the loss of hospital-based SNF beds has increased to 43.3% and is already here, perhaps five years early.]
Between 2013 and 2015 San Francisco lost 265 licensed SNF beds in acute-care hospitals, and the report indicates San Francisco may lose another 56 SNF beds in acute-care hospitals in the five years between 2015 and 2020, just four years from now. Is it realistic to believe that 265 acute-care SNF beds were lost over a three-year period, but only 56 acute-care SNF beds will be lost over a five-year period?
 Tack on the loss
of another 151 beds in “freestanding” (i.e., non-hospital-based)
SNF beds, from 1,374 to 1,223 in the 12 years between 2002 and
2014, which represents an additional 9% decline in SNF-bed capacity.
Tack on the loss
of another 151 beds in “freestanding” (i.e., non-hospital-based)
SNF beds, from 1,374 to 1,223 in the 12 years between 2002 and
2014, which represents an additional 9% decline in SNF-bed capacity.
The report documents the loss of 16 “board and care” care facilities and 80 Residential Care Facilities for the Elderly beds that have closed in the past five years, since 2011.
The report also documents San Francisco faces a 1,745-bed SNF gap between supply and demand within the next 14 years, by 2030, in part because San Franciscans aged 65 and older will comprise 20% of San Francisco’s population by 2030, increasing by 69.9% between 2016 and 2030 — from 113,000 now to 192,000 in those 14 short years.
The report again discusses the probability of having unmet skilled nursing needs in San Francisco, and bemoans the fact that “some patients prefer to be placed [discharged] in San Francisco, which increases the wait time [to discharge] compared to out-of-county placement” discharges.
 Jeesh! SNF-bed
advocates have been telling DPH, the LTCCC, and other City officials
for years that 1) Some patients prefer placement in a SNF, rather
than “community based services and supports,” and 2)
Many patients do not want to be discharged
out-of-county, both significant patient preferences the City has
all but chosen to ignore during “planning”!
Jeesh! SNF-bed
advocates have been telling DPH, the LTCCC, and other City officials
for years that 1) Some patients prefer placement in a SNF, rather
than “community based services and supports,” and 2)
Many patients do not want to be discharged
out-of-county, both significant patient preferences the City has
all but chosen to ignore during “planning”!
San Francisco hospitals involved in the “Post-Acute Care Shortage” report cited out-of-county discharges as being “necessary” to move certain patients out of acute care into lower levels of care, including subacute patients; Medi-Cal patients, particularly those needing long-term bed placement; and patients with behavioral difficulties. But the report never stratified by hospital how many out-of-county placements have occurred, nor a combined aggregate number of out-of-county placements that may have already been made by San Francisco’s private-sector hospitals.
In addition to the surge in the number of elderly over the age of 65 nationwide, the report also notes that post-acute care across the country will be shaped by the prevalence of chronic illnesses among the elderly that is also expected to increase. By 2020 — just four short years from now — the number of Americans with chronic illnesses such as congestive heart failure, diabetes, COPD, and Alzheimer’s is projected to grow from 133 million to 157 million, an 18% increase, with 81 million having multiple chronic conditions.
Nationwide, between 2010 and 2050, the number of people 65 and older who have Alzheimer’s face a 193.6% increase, from 4.7 million to 13.8 million. And the number of people over age 65 nationwide who have or will develop Alzheimer’s is expected to increase 40% just between 2015 and 2025 — which is just nine years away.
 Where will Alzheimer’s
patients in San Francisco who are unable to live safely in the
community be cared for, since San Francisco officials have done
a completely lousy job of planning for long-term SNF care, even
after knowing about the impending tsunami of people with Alzheimer’s
in San Francisco?
Where will Alzheimer’s
patients in San Francisco who are unable to live safely in the
community be cared for, since San Francisco officials have done
a completely lousy job of planning for long-term SNF care, even
after knowing about the impending tsunami of people with Alzheimer’s
in San Francisco?
Of note, in October 2017 Medicare’s Nursing Home Compare website will start publicly reporting the number of patients discharged to skilled nursing facilities that are then re-admitted to hospitals, and beginning in 2019 skilled nursing facilities will be penalized for hospital re-admissions. Notably, Medicare may not have gone far enough in deciding which facilities should be penalized for hospital re-admissions, since potentially premature discharges from acute-care facilities to SNF’s may involve discharges bound to fail, requiring hospital re-admission. Medicare should also hold acute care hospitals to the same standard and penalize them financially for making any premature discharges to SNF’s that occur.
So the push is on SNF’s to do what they can to prevent hospital re-admissions.
 Among short- and
long-term recommendations contained in the report, one claims
the City should:
Among short- and
long-term recommendations contained in the report, one claims
the City should:
This is comical precisely because the Mayor’s Long-Term Care Coordinating Council (LTCCC) was created 12 years ago charged with the task of identifying the number of long-term SNF patients that could safely be served with “community-based services and supports” rather than needing placement in a SNF. Over those 12 years, it appears the LTCCC has failed miserably at obtaining an accurate count of the total number of long-term care SNF patients who could be served in the community, instead. Why is this taking so long to assess?
Another recommendation calls for exploring new incentives and funding options to address current gaps in facility-based care and bringing new skilled nursing facilities, Residential Care Facilities for the Elderly, and subacute facilities into the market, a long-overdue admission that more facilities need to be added to address pent-up demand for these levels of care.
 A companion recommendation
“encourages” acute-care hospitals to work with a SNF
provider to open a SNF unit funded by all City hospitals, with
each hospital to have a certain number of SNF beds in a combined
facility. Shouldn’t these private-sector hospitals have considered
this previously as an option, perhaps with the help of the Hospital
Council of Northern and Central California, before collectively
shedding their in-house SNF units?
A companion recommendation
“encourages” acute-care hospitals to work with a SNF
provider to open a SNF unit funded by all City hospitals, with
each hospital to have a certain number of SNF beds in a combined
facility. Shouldn’t these private-sector hospitals have considered
this previously as an option, perhaps with the help of the Hospital
Council of Northern and Central California, before collectively
shedding their in-house SNF units?
The report also suggests “encouraging” SNF providers to build new, or upgrade existing, facilities, with a percentage of beds reserved for difficult-to-place populations. Why has it taken so long to come up with this common-sense recommendation after all these years?
Another recommendation calls for exploring public-private partnerships to support alternative post-acute care settings, but that recommendation failed to stipulate that the new post-acute care settings need to be placed in San Francisco, not out-of-county.
Media Coverage of New Report
 Following presentation
of the “Post-Acute Care Shortage” report to the
Health Commission, the San Francisco Chronicle appears
to have published not one story about it, although I could be
wrong.
Following presentation
of the “Post-Acute Care Shortage” report to the
Health Commission, the San Francisco Chronicle appears
to have published not one story about it, although I could be
wrong.
To its credit, the San Francisco Examiner published an article by Joshua Sabatini on February 19, 2016 discussing the “Post-Acute Care Shortage” report presented to the Health Commission of February 16. Unfortunately, Sabatini’s article failed to place the story in perspective on a variety of levels.
First, Sabatini quoted Sneha Patil, a Health Program Planner in DPH’s Office of Policy and Planning, saying that “San Francisco is at risk for an inadequate supply of skilled nursing beds in the future” to inform the Health Commission. But Sabatini didn’t place into context that the Health Commission had previously been warned that the shortage of SNF beds in the City will lead to, or has already led to, an unmet need for skilled nursing level of care in the City.
It’s not just that there is an inadequate supply to meet demand. It’s that the need for demand isn’t being met after years of inadequate and poor planning. How long is an unmet need going to take before the Health Commission “gets” the need?
 Second, Sabatini
reports that “health officials are attempting”
to reverse the supply of beds that have decreased in recent
years, by “working with hospital officials and other health
care service providers.” There is no evidence whatsoever
that any efforts have been made to reverse the supply of lost
beds, either by Health Department officials, or other health care
providers, or that their combined efforts have been successful,
or even gotten off the ground.
Second, Sabatini
reports that “health officials are attempting”
to reverse the supply of beds that have decreased in recent
years, by “working with hospital officials and other health
care service providers.” There is no evidence whatsoever
that any efforts have been made to reverse the supply of lost
beds, either by Health Department officials, or other health care
providers, or that their combined efforts have been successful,
or even gotten off the ground.
Third, Health Commissioner David Pating, MD — a psychiatrist and Chief of Addiction Medicine at Kaiser Medical Center in San Francisco who was appointed by Mayor Ed Lee to the Health Commission in September 2014 — appears to be completely clueless about the severe SNF bed shortage that has been looming long before he was appointed to the Health Commission. To be fair, Pating wasn’t appointed to the Health Commission until after the Commission had concluded in June 2014 that closure of CPMC’s SNF units would have a detrimental effect on the level of SNF care in San Francisco.
But Pating had to have known the Health Commission had made this ruling three months before he was appointed to the Health Commission.
 Sabatini quoted Pating
as saying San Francisco “has a gap here that is looking to
be solved.”
Sabatini quoted Pating
as saying San Francisco “has a gap here that is looking to
be solved.”
Golly, Dr. Pating, no kidding? The SNF-bed “gap” has been brewing for decades, and has been looking to be solved the whole time! That would be the whole time that the Health Commission has turned a blind eye to the need for SNF beds.
Sabatini further quoted Commissioner Pating as saying:
Pating is kidding, right?
Does he not know that the City owns 62 acres on the grounds of Laguna Honda Hospital where there is plenty of room to build more SNF beds (since, in fact, another 420 SNF beds that had been planned to fit on LHH’s campus were simply eliminated, largely due to the cost overruns of the new facility)? Since the City already owns that land, there would be no additional cost to acquire property on which to build out more SNF beds. Pating also appears to be ignoring there is a glut of space in Mission Bay that could be pressed into service to build additional SNF beds.
 Nowhere in Sabatini’s
article does he explicitly mention the new report shows on page
14 that the projected gap in skilled nursing beds will reach a
1,745-bed shortage just 14 years from now in 2030. This isn’t
about a 500-bed, or a 1,000-bed, shortage Pating babbled about.
It’s almost double that, at a 1,745-bed shortage, a number
you’d think an MD with eight or more years of medical school
could wrap his mind around.
Nowhere in Sabatini’s
article does he explicitly mention the new report shows on page
14 that the projected gap in skilled nursing beds will reach a
1,745-bed shortage just 14 years from now in 2030. This isn’t
about a 500-bed, or a 1,000-bed, shortage Pating babbled about.
It’s almost double that, at a 1,745-bed shortage, a number
you’d think an MD with eight or more years of medical school
could wrap his mind around.
Given multiple studies (discussed below) pointing to the need for more SNF beds, how can Pating remain “unclear” about how many additional SNF beds are needed? The new report clearly shows the City may be short 1,745 SNF beds over the next 14 years. Did Pating simply ignore the “expert” analyses provided by DPH’s Sneha Patil, DPH’s Colleen Chawla, the Hospital Council of Northern and Central California, and the study conducted on behalf of the Chinese Hospital Association of San Francisco?
Even worse, Pating stuck his foot in his mouth when Sabatini quoted him as saying:
 Really, Dr. Pating?
More out-of-county patient dumping, including elderly and disabled
San Franciscans who simply need long-term care skilled nursing
care? Pating also informed Sabtini that hospital officials have
difficulty in placing patients in sub-acute care beds. Pating
said:
Really, Dr. Pating?
More out-of-county patient dumping, including elderly and disabled
San Franciscans who simply need long-term care skilled nursing
care? Pating also informed Sabtini that hospital officials have
difficulty in placing patients in sub-acute care beds. Pating
said:
How is Pating aware of discharges at the level of Los Angeles County? What else does Pating know, but isn’t telling us, about the severity of out-of-county discharges? How’s that for a Commissioner charged with supporting the San Francisco Department of Public Health’s mission to protect and promote the health of all San Franciscans?
Simple. Just dump them out-of-county, problem solved. Thanks, Dr. Pating!
 Is that why Mayor
Ed Lee appointed Pating to the Health Commission in 2014? To simply
get rid of the “expense” side of the equation, not the
“care” side?
Is that why Mayor
Ed Lee appointed Pating to the Health Commission in 2014? To simply
get rid of the “expense” side of the equation, not the
“care” side?
Fourth, Sabatini reported in the Examiner that Abbie Yant, St. Francis Memorial Hospital’s Vice President for Mission, Advocacy and Community Health, said that the new “Post-Acute Care Shortage” report “represents the first time The City is addressing post-acute care at large.” Yant went on to babble “We need to protect what we now have. The problem is here today. We do have some urgency around that.”
Gee, Ms. Yant, what a refreshing admission from you that this is the first time the City has gotten around to addressing post-acute care needs, 20 years or more into the crisis!
If Yant truly believes that we “need to protect what we now have,” why did she advocate in 2015 on behalf of St. Mary’s to close its SNF beds? After all, Yant has served on the Mayor’s Long-Term Care Coordinating Council (LTCCC ) since being first appointed to it on January 1, 2011, and during the five years she has served on the LTCCC she didn’t lift a finger to stop the closure of 90 SNF beds between St. Francis, CPMC, and St. Mary’s.
On the “protect-what-we-now-have” front, Yant was missing in action to protect SNF beds that “we had before.” Why didn’t she do more to protect “what we had previously” during her five years on the LTCCC?
 The problem she described
as being “here today” has been going on since at least
2007, if not before. Where has Ms. Yant been all of this time?
It appears to be the same message lost on Health Commissioner
Pating.
The problem she described
as being “here today” has been going on since at least
2007, if not before. Where has Ms. Yant been all of this time?
It appears to be the same message lost on Health Commissioner
Pating.
Previous Reporting: Slouching Towards Unmet SNF Needs
Despite a soaring population of elderly San Franciscans, the City has no plans on where to provide long-term care for them given a severe, and worsening, skilled nursing facility bed shortage. And the City has irresponsibly engaged in no planning to mitigate the bed shortage.
This was no accident. The Health Commission and the City have engaged in a pretense since at least 2004 — when then-Mayor Gavin Newsom formed the LTCCC — that they have been actively planning to address long-term care needs for the City’s elderly. It’s time to drop the pretense and admit their “plan” — or more accurately, their complete lack of planning — has been craven, all along.
 In “Laguna
Honda Hospital: Pot-bellies vs. Beds?” (July 2009), I noted that in March 2005, then-Health
Commission president Lee Ann Monfredini requested that then-Director
of Public Health, Mitch Katz, update his 1998 White Paper
regarding needs for long-term care skilled nursing facility (SNF)
beds. Now 11 years after Monfredini requested an update, the Department
of Public Health still hasn’t produced an updated White
Paper, which now hasn’t been updated in over 18 years.
In “Laguna
Honda Hospital: Pot-bellies vs. Beds?” (July 2009), I noted that in March 2005, then-Health
Commission president Lee Ann Monfredini requested that then-Director
of Public Health, Mitch Katz, update his 1998 White Paper
regarding needs for long-term care skilled nursing facility (SNF)
beds. Now 11 years after Monfredini requested an update, the Department
of Public Health still hasn’t produced an updated White
Paper, which now hasn’t been updated in over 18 years.
Similarly, in May 1997 the Hospital Council of Northern and Central California authored its San Francisco Nursing Facility Bed Study, which also hasn’t been updated in 19 years. Both studies had predicted San Francisco faced a potential 4,207 SNF-bed deficit by 2020, just four years from now.
I also reported in “Pot-bellies vs. Beds?” that on June 11, 2009, San Francisco’s Long Term Care Coordinating Council (LTCCC) — whose mission claims it will guide the development of an integrated system of home, community-based, and institutional services for older adults and adults with disabilities — passed a resolution resolving that CPMC not close “any of its 101 post-acute skilled nursing beds, either in 2010 or later, until reasonable alternatives are established.”
The LTCCC’s 2009 resolution also called on the City to explore “the need for citywide health planning that considers San Francisco’s demand for acute care beds and services, alternatives for acute care beds, post-acute care beds and services, rehabilitation services, and transitional care.” The LTCCC pointedly eliminated from its draft resolution a call for planning for SNF level of care, an obvious planning need, and also eliminated from its final resolution a statement contained in its June 3 initial draft that said CMPC’s plans “will have a significant and negative impact on the overall availability” of SNF beds for vulnerable adults.
 Fast forward five
years. On June 15, 2014 the San Francisco Health Commission adopted
Resolution 14–8 which determined that
the closure of 24 skilled nursing facility beds at California
Pacific Medical Center “will have a
detrimental impact on the health care services in the community.”
And during those five years between the LTCCC’s resolution
and the Health Commission’s resolution, there appears to
have been no citywide healthcare planning
across multiple City departments at all, and no efforts to create
alternatives for post-acute care beds.
Fast forward five
years. On June 15, 2014 the San Francisco Health Commission adopted
Resolution 14–8 which determined that
the closure of 24 skilled nursing facility beds at California
Pacific Medical Center “will have a
detrimental impact on the health care services in the community.”
And during those five years between the LTCCC’s resolution
and the Health Commission’s resolution, there appears to
have been no citywide healthcare planning
across multiple City departments at all, and no efforts to create
alternatives for post-acute care beds.
In “Who’s Dumping Grandma?” (June 2013), I noted there are many stories of patients needing skilled nursing care who are being dumped out of county, and asked why City Attorney Dennis Herrera doesn’t seem concerned about the dumping of skilled nursing patients out of county.
“Who’s Dumping Grandma?” focused heavily on the reconfiguration of the Department of Public Health’s “Mental Health Rehabilitation Facility” (MHRF) built on the grounds of SFGH, which was later renamed the “Behavioral Health Center” (BHC) in order to be more politically correct.
The fate of the MHRF is relevant precisely because the new “Post-Acute Care Shortage” report frets about increasing out-of-county placements of so-called “vulnerable patients,” including those who have behavioral problems caused by mental health disorders and mental illnesses, progressive dementia’s, traumatic brain injuries, or are abusing substances, all of whom are inherently difficult to place in skilled nursing facilities, given the lack of such facilities in San Francisco. Factor in patients with degenerative Alzheimer’s who require increasing levels of supervision and personal care, who are also difficult-to-place vulnerable people.
A bond measure to build the MHRF/BHC as a “mental health skilled nursing center,” was passed in November 1987 but it took nine years before the MHRF was built and opened in 1996. The MHRF cost $39.7 million to build, including paying interest on the bond.
The bond measure’s supporters asserted building the MHRF as a long-term care facility for the mentally ill would close a gap in San Francisco’s mental health care system, and would permit patients to remain near friends and families to facilitate recovery.
Just seven short years after the MHRF opened, a so-called “Blue Ribbon Committee” split the three-story MHRF into multiple uses in 2003, reducing the 147 psychiatric beds to just 47 by 2008. Five years later, DPH budget initiative “B–1” for FY 2013–2014 — apparently with approval of San Francisco’s Health Commission — proposed converting one wing of the third floor at the MHRF/BHC to add 23 “respite” beds by cutting the MHRF’s psychiatric beds from 47 down to just 24. DPH proposed “re-configuring” the MHRF into a residential care and respite care facility, and transferring 34 “behavioral health patients” to Laguna Honda Hospital.
 DPH proposed closing
the Skilled Nursing Facility (SNF) on the MHRF’s second floor
and replacing it with a Residential Care Facility for the Elderly
(RCFE), changing the 34 SNF beds to 57 RCFE beds, and converting
single-rooms into shared two-person rooms. Although DPH claimed
there would be no change to the first floor, 22 of the 41 Adult
Residential Care Facility (RCF) beds on the first floor were to
be re-licensed as RCFE beds. DPH asserted the 79 RCFE beds would
be used for non-ambulatory patients.
DPH proposed closing
the Skilled Nursing Facility (SNF) on the MHRF’s second floor
and replacing it with a Residential Care Facility for the Elderly
(RCFE), changing the 34 SNF beds to 57 RCFE beds, and converting
single-rooms into shared two-person rooms. Although DPH claimed
there would be no change to the first floor, 22 of the 41 Adult
Residential Care Facility (RCF) beds on the first floor were to
be re-licensed as RCFE beds. DPH asserted the 79 RCFE beds would
be used for non-ambulatory patients.
On April 6, 2014, the Department of Public Health submitted an “innovation project” proposal to Mayor Ed Lee — “Work Plan #: INN–17,” with “INN” apparently referring to “innovation” — to create a facility at SFGH to:
Work Plan #: INN–17 proposed a budget of $500,400 annually in each of the first four years for operating expenses, but included no sources of revenue for the $500,400 in expenditures that would total $2 million in its first four years.
 The facility —
named “Hummingbird Place Peer Respite” —
occupies the first floor of the three-story Behavioral Health
Center (MHRF/BHC) as some sort of psychiatric service. Hummingbird
Place appears to have displaced the 41 “Adult Residential
Care Facility” (RCF) and “Residential Care Facility
for the Elderly” (RCFE) beds on the first floor of the MHRF/BHC.
The second and third floors were reportedly to continue housing
two residential programs.
The facility —
named “Hummingbird Place Peer Respite” —
occupies the first floor of the three-story Behavioral Health
Center (MHRF/BHC) as some sort of psychiatric service. Hummingbird
Place appears to have displaced the 41 “Adult Residential
Care Facility” (RCF) and “Residential Care Facility
for the Elderly” (RCFE) beds on the first floor of the MHRF/BHC.
The second and third floors were reportedly to continue housing
two residential programs.
One goal of the Hummingbird Place program appears to be to lessen strain on SFGH’s “Psychiatric Emergency Services” (PES) beds, since PES beds have also been severely slashed — by design — over the past decades.
Although the February 16 “Post-Acute Care Shortage” report bemoans the loss of board-and-care and RCFE facilities — reporting that approximately 16 board-and-care facilities and 80 RCFE beds have closed since 2011 — the new report mentions not one word about the closure of the MHRF/BHC center’s RCFE beds for the elderly, or the conversion of the RCFE beds to respite care.
What kind of “innovation” is it that converts short-supply RCFE beds for the elderly — forcing elderly and non-ambulatory San Franciscans needing residential care into out-of-county discharges — into “respite” care for those who are “not quite ready to engage in mental health treatment,” instead?
Hummingbird Place reportedly opened on April 20, 2015 with “Innovation Mayor” Ed Lee and Director of Public Health Barbara Garcia in attendance. The respite program supposedly functions as a daytime, closed referral center. It is not yet known how many “beds” or clients were (or are) to be served at Hummingbird Place.
After spending $40 million of taxpayer funds to build the MHRF/BHC, DPH has converted use of the facility so many times that the $40 million appears to have gone up in smoke.
According to its web site, SFGH reported that beginning in FY 2015–2016 (which began in July 2015), it no longer operates the MHRF/Behavioral Health Center on the campus of SFGH. DPH confirmed for this article that it — the Department of Public Health and its “Transitions” Program and its Behavioral Health Branch, not SFGH — operates both the MHRF/BHC and Hummingbird Place on the first floor of the BHC facility.
Dys-Integration of ‘Old Friends’
 In “The Big
Squeeze: Dys-Integration of ’Old Friends’ (July 2014),” I covered the crisis in
long-term care skilled nursing beds in San Francisco and included
data presented by San Francisco’s Department of Public Health
to the Health Commission, data that appears to have been totally
ignored over the past two years.
In “The Big
Squeeze: Dys-Integration of ’Old Friends’ (July 2014),” I covered the crisis in
long-term care skilled nursing beds in San Francisco and included
data presented by San Francisco’s Department of Public Health
to the Health Commission, data that appears to have been totally
ignored over the past two years.
In 2014, San Francisco’s Health Commission and the Department of Public Health relied on a May 2011 analysis prepared by Resource Development Associates prepared for the Chinese Hospital Association of San Francisco that the Department of Public Health DPH had commissioned — an analysis now five years old, and wildly out of date — which then projected a 700-bed skilled nursing facility (SNF) shortage in San Francisco by 2050, 40 years from the time the 2011 analysis was prepared. Of note, Health Commission president Edward Chow is affiliated with San Francisco’s Chinese Hospital; Chow had to have known of this 700-bed shortage all along, but has turned a blind eye to the problem.
Since the Resource Development Associates’ 2011 analysis is so sadly out of date, is the 700-bed shortage now much worse?
Given that the February 2016 report “Framing San Francisco’s Post-Acute Care Shortage” just presented to the Health Commission now claims demand for SNF beds may reach 4,287 beds by 2030 and San Francisco currently only has 2,542 SNF beds, it is clearer that San Francisco may have a 1,745-bed SNF gap by 2030, not a 700-bed gap by 2050.
How did this gap escalate in the two years since 2014 by 1,000 beds — from a purported 700-bed shortage to a new projection of a 1,745-bed shortage — a gap that has widened 20 years earlier than the year 2050?
 Of interest, when
the Health Commission was presented with data in 2014 regarding
the closure of CPMC’s SNF beds, no data was presented to
it indicating what becomes of patients who require long-term rehabilitation
longer than 60 days, and whether those rehab patients are diverted
to the few remaining facilities that provide longer-term rehabilitation.
And the February 2016 “Framing San Francisco’s Post-Acute
Care Shortage” report mentioned nothing about patients
needing long-term care rehabilitation services longer than 60
days, and where they go for care.
Of interest, when
the Health Commission was presented with data in 2014 regarding
the closure of CPMC’s SNF beds, no data was presented to
it indicating what becomes of patients who require long-term rehabilitation
longer than 60 days, and whether those rehab patients are diverted
to the few remaining facilities that provide longer-term rehabilitation.
And the February 2016 “Framing San Francisco’s Post-Acute
Care Shortage” report mentioned nothing about patients
needing long-term care rehabilitation services longer than 60
days, and where they go for care.
For her part, Colleen Chawla, DPH’s Deputy Director and Director of Policy and Planning, presented a memo to the Health Commission on June 12, 2014 that indicated a report issued in 2012 by San Francisco’s Department of Aging and Adult Services reported that:
Chawla went on to note:
The HCSMP was developed by the San Francisco Planning Department and the Department of Public Health and was adopted in October 2013, documenting a clear and increasing need for SNF beds in San Francisco.
But it wasn’t until 2015, that Chawla and the Health Department finally got around to admitting during the “Prop. Q” hearing on St. Mary’s closure of its SNF unit that the decades-long, on-going loss of SNF beds in San Francisco would result in un-met skilled nursing needs for San Franciscans. We’re now there, with un-met SNF needs that will worsen.
Detrimental Skilled Nursing Cuts
 In “Detrimental
Skilled Nursing Cuts” (June 2015), I covered the long-term care skilled
nursing bed shortage, reporting several disturbing issues.
In “Detrimental
Skilled Nursing Cuts” (June 2015), I covered the long-term care skilled
nursing bed shortage, reporting several disturbing issues.
An April 19, 2015 Health Department analysis provided to the Health Commission regarding St. Mary’s proposed SNF bed closure failed to clearly point out that between 2013 and 2020, DPH projected an additional loss of 346 hospital-based SNF beds.
A separate April 29, 2015 Department of Public Health memo from Ms. Patil projected that hospital-based skilled nursing facility beds will have declined from 2,166 beds in 2002 to just 1,240 beds in 2020 — a whopping 42.8% decline and loss of 926 hospital-based SNF beds.
Of those, fully 90 of the hospital-based SNF beds closed between 2007 and 2015 occurred in just three hospitals that faced “Prop. Q” hearings before the Health Commission.
The remaining 836 (of 926) hospital-based SNF bed closed apparently were never considered during Health Commission “Prop. Q” hearings. How did that happen? Did the Health Commission simply look the other way?
 Ms. Patil repeated
in April 2015 that the industry trend of converting long-term
SNF beds to short-term SNF beds means that “any reduction
of SNF beds, regardless of type, creates an overall capacity risk
for San Francisco and is likely to have a detrimental impact.”
Patil noted that any reduction of hospital-based SNF beds needs
to be offset by increasing the availability of community-based
post-acute care alternatives to preserve and maintain “capacity.”
Ms. Patil repeated
in April 2015 that the industry trend of converting long-term
SNF beds to short-term SNF beds means that “any reduction
of SNF beds, regardless of type, creates an overall capacity risk
for San Francisco and is likely to have a detrimental impact.”
Patil noted that any reduction of hospital-based SNF beds needs
to be offset by increasing the availability of community-based
post-acute care alternatives to preserve and maintain “capacity.”
Patil also noted that “as hospital-based short-term SNF beds close, this may impact the availability of long-term SNF beds for which there is already a long wait list in San Francisco and the Bay Area.”
A “Resolved” statement in the Resolution the Health Commission adopted regarding closure of St. Mary’s SNF beds was proposed to say:
But cleverly, David Singer, the Health Commission’s Vice President, proposed a friendly amendment designed to tone down whether there would be unmet skilled nursing needs; he proposed moving the “unmet” clause to the end of the sentence. The first “Resolved” statement that was eventually passed was changed to read:
 Why Singer felt moving
the “unmet needs” clause to the end of the sentence
was so critical is unknown. It really didn’t matter where
the “unmet” phrase was placed in the sentence. “Unmet,”
still means “unmet,” despite Singer’s spin control.
Why Singer felt moving
the “unmet needs” clause to the end of the sentence
was so critical is unknown. It really didn’t matter where
the “unmet” phrase was placed in the sentence. “Unmet,”
still means “unmet,” despite Singer’s spin control.
A “Whereas” clause in the Resolution indicated that “while institutional [hospital-based] post-acute care continues to decrease, the availability of community-based post-acute care will need to rise to maintain the capacity to care for San Francisco’s population.”
For his part, Health Commissioner Edward Chow noted in April 2015 that back in 2007 during the “Prop. Q” hearing on the closure of St. Francis Hospital’s SNF units (found to have been detrimental) the Health Commission had asked for a study on SNF bed needs in San Francisco. It took DPH until February 2016 — fully nine years — to obtain any sort of SNF bed study when it received the “Framing San Francisco’s Post-Acute Care Shortage” report on February 16, 2016.
How much foot dragging occurred during that nine-year wait? Why didn’t the Health Commission push harder during that nine-year period to obtain new data?
It was clear during the Health Commission’s May 19, 2015 hearing that the Commission didn’t seem to understand DPH’s concern that shifting post-acute care hospital-based SNF care to short-term community SNF beds would have an immediate detrimental impact then — and now — not ten years in the future.
 Clearly, no community-based
post-acute care alternatives have been created since 2015, or
created earlier. Post-acute care alternatives haven’t surfaced
to maintain capacity, despite the wishful thinking of the Health
Commission.
Clearly, no community-based
post-acute care alternatives have been created since 2015, or
created earlier. Post-acute care alternatives haven’t surfaced
to maintain capacity, despite the wishful thinking of the Health
Commission.
Laguna Honda Hospital’s “Mission” Changed Again
Just before San Francisco’s Public Health Commission debated the new report on February 16, 2016 about the critical shortage of skilled nursing care beds to care for San Francisco’s quickly increasing population of elderly residents, a Health Commission subcommittee called the Laguna Honda Hospital Joint Conference Committee (LHH-JCC) quietly changed Laguna Honda’s mission statement from providing long-term care to focus on providing “post-acute care” services, instead.
It’s not a mere shift in semantics.
It’s much more profound, because it allows LHH and DPH to determine which post-acute care services LHH will offer, and it may allow the hospital to say, “Our mission isn’t to provide long-term skilled nursing care so we’re not going to admit you and you should go shop elsewhere, even if it means out-of-county placement.”
Knowing in advance of its full Commission meeting that it was to be presented with a new report on February 16 that acknowledges San Franciscans aged 65 and older will increase by 69.9% between 2016 and 2030 — from 113,000 now to 192,000 in the 14 short years leading up to 2030 — and knowing that the new report would document an increasingly severe SNF bed shortage to care for frail elderly San Franciscans, the LHH-JCC quietly changed LHH’s mission statement a month earlier on January 12, and did so without providing adequate public notice of what it was about to do.
Laguna Honda’ mission statement has been changed seven times since it was first adopted in May 1992, including being revised four times since October 2007 alone.
LHH’s initial mission statement adopted on May 20, 1992 stated unequivocally that LHH’s mission would focus on long-term care for the elderly and disabled:
Among the goals listed in initial the 1992 mission statement, one goal stated the hospital would maintain within LHH’s resident population appropriate proportions of patients at all levels of skilled nursing care so LHH could be a comprehensive skilled nursing facility.
Fifteen years later, the Health Commission adopted Resolution 06–07 on June 5, 2007 that read, in part, that the Commission would adopt Laguna Honda’s FY 2007–2008 Strategic Plan, including:
 Although the Health
Commission adopted Resolution 06–07, for some unexplained
reason that mission change is not listed among the historical
list of changes to LHH’s Policy 01–00, its mission statement.
Although the Health
Commission adopted Resolution 06–07, for some unexplained
reason that mission change is not listed among the historical
list of changes to LHH’s Policy 01–00, its mission statement.
But LHH’s mission statement adopted seven years ago on October 27, 2009 — long before the LHH replacement hospital opened in 2010 — included language that LHH was to be an “innovative world-class center of excellence in long-term care and rehabilitation” … the very mission that the City had sold to voters who approved the 1999 bond measure to rebuild LHH as a skilled nursing facility.
LHH’s new mission statement adopted on January 12, 2016 changed LHH’s mission from caring for long- and short-term care patients to LHH becoming a “leader in post-acute care.” And completely absent from the January 2016 revised mission statement is any mention of long-term care, short-term care, or rehabilitation services, all of which have now been completely excised from LHH’s mission statement.
Over the 24-year period since LHH first adopted its mission statement in 1992 to provide long-term care for elderly and disabled San Franciscans, the mission statement has completely morphed into providing “post-acute care,” rather than long-term care, a bait-and-switch if there ever was one.
 And the most recent
revision in January 2016 was hampered by inadequate notice to
members of the public about what was about to transpire. Although
the Department of Public Health’s executive secretary to
the Health Commission distributed an agenda in advance of the
January 12 Health Commission’s LHH-JCC sub-committee meeting
to DPH’s “interested persons” e-mail list, the
subject line of the e-mail indicted the meeting was for the full
Health Commission, not the LHH-JCC sub-committee, depriving members
of the public from knowing from the subject line that it was the
JCC that was meeting, not the full Commission.
And the most recent
revision in January 2016 was hampered by inadequate notice to
members of the public about what was about to transpire. Although
the Department of Public Health’s executive secretary to
the Health Commission distributed an agenda in advance of the
January 12 Health Commission’s LHH-JCC sub-committee meeting
to DPH’s “interested persons” e-mail list, the
subject line of the e-mail indicted the meeting was for the full
Health Commission, not the LHH-JCC sub-committee, depriving members
of the public from knowing from the subject line that it was the
JCC that was meeting, not the full Commission.
After the fact, a records request produced the LHH-JCC’s January 12 agenda, which did not include a separate agenda item on changing LHH’s mission statement, so interested persons would learn that LHH’s mission statement was being tinkered with, yet again. Instead, the mission statement change appears to have been lumped together in a single agenda item titled “Consideration of Changes to Hospital-Wide Policies & Procedures” [sic: “hospitalwide”], and the agenda failed to list which policies were being considered for revisions.
Unfortunately, the Health Commission’s current procedure posts background explanatory documents for given agenda items only on-line, and only for a brief period of time. Following any given meeting, hyperlinks to the supplemental background files are no longer available on the Health Commission’s web site. Neither the agenda retained on-line following a given meeting, nor the meeting’s minutes eventually posted on-line, include a list of which hospitalwide policies were considered, changed, and approved during meetings, and the hyperlinks to background files vanish.
Of note, the LHH-JCC meeting minutes from its January 12, 2016 meeting reported absolutely no discussion at all by the Health Commissioners appointed to the LHH-JCC of the proposed changes to LHH’s mission statement to focus on post-acute care. It apparently passed the changes to the mission statement in the absence of any discussion whatsoever. If there may have been a verbal discussion of LHH’s mission change, that discussion was excised from the meeting minutes.
 Decades of Planning Up in Smoke
Decades of Planning Up in Smoke
As far back as 1982, healthcare planners nationwide knew about the looming severe shortage of skilled nursing beds all over the country. For example, an October 1982 New York Times article titled “Nursing Home Bed Shortage Grows With Number of Aged” noted that health officials reported a shortage of nursing home beds in many parts of the country, and the officials said the problem would grow worse as the elderly population increases over the next few decades. The NYT article noted:
Now 33-and-a-half-years following the Times article, we’re back to the future with the exact same problem: The supply of SNF beds still isn’t meeting the demand for this level of care, particularly not in San Francisco.
 It’s as if four
decades of planning has gone up in smoke.
It’s as if four
decades of planning has gone up in smoke.
History of Planning to Rebuild LHH
Planning to rebuild Laguna Honda Hospital and Rehabilitation Center (LHH) began in 1980. After 19 years of studies, community debates, and development of an Institutional Master Plan and a four-volume Facility Master Plan that received approval of the Department of Public Health and the Planning Department, San Francisco voters in 1999 were asked to authorize a bond measure for LHH to be rebuilt as a healthcare facility providing long-term skilled nursing care. Seventy-three percent of voters approved the $299 million bond measure to rebuild LHH to safely care for poor, elderly, and physically disabled San Franciscans.
Following passage of the bond in 1999, it took another 11 years before the replacement hospital was constructed and opened in 2010. Between the time planning first began in 1980 and when LHH’s new facility opened, fully 30 years had slipped away; that was now six years ago, bringing us to a 36-year period.
 Now in 2016, the
Department of Public Health and San Francisco’s Public Health
Commission continues to drag its feet planning for skilled nursing
care needs of elderly San Franciscans, fully 36 years after the
planning for LHH began in 1980. And we’re now at the exact
same point we were almost 40 years ago — with an insufficient
number of SNF beds to care for San Francisco’s rapidly aging
population and disabled people.
Now in 2016, the
Department of Public Health and San Francisco’s Public Health
Commission continues to drag its feet planning for skilled nursing
care needs of elderly San Franciscans, fully 36 years after the
planning for LHH began in 1980. And we’re now at the exact
same point we were almost 40 years ago — with an insufficient
number of SNF beds to care for San Francisco’s rapidly aging
population and disabled people.
Health Commissioners who have dragged their feet include current Health Commissioner Edward Chow, who was first appointed to the Health Commission in 1989 for a one-year term, and has been reappointed so many times he has now served on the Health Commission for 27 years. Health Commissioner David Sanchez was first appointed in 1997, and has now served for 19 years on the Commission.
Both men have served during the same decades that the four-decade-long SNF crisis in San Francisco has brewed. Both men should know how long it takes to get additional capacity and facilities built, but neither man has done anything in their 20+-years on the Health Commission to get additional SNF beds built, or stop the loss of SNF and other post-acute care beds citywide.
 Both men squandered
decades with insufficient planning to ensure an adequate supply
of SNF beds are available in San Francisco to meet the demand.
They had to have known this the whole time they’ve served
on the Health Commission.
Both men squandered
decades with insufficient planning to ensure an adequate supply
of SNF beds are available in San Francisco to meet the demand.
They had to have known this the whole time they’ve served
on the Health Commission.
Failure of the Long-Term Care Coordinating Council and Its “Community Living Fund”
In November 2004, then-Mayor Gavin Newsom created a 40-member Long Term Care Coordinating Council (LTCCC) to provide policy guidance to the Mayor’s Office to implement and monitor community-based long term care planning in San Francisco, and facilitate improved coordination of home, community-based, and institutional services for older adults and adults with disabilities.
Nearly 12 years later, the LTCCC has done little to provide long-term care in community-based facilities, and has little to show for its efforts. Just ask Abbie Yant, or SNF-bed obstructionist Herb Levine, who also served on the LTCCC and who once told me — with a straight face, albeit smugly — that with the right amount of community-based “services and supports” in place in-lieu of nursing homes, there would be a need for zero SNF beds at Laguna Honda Hospital.
 While the LTCCC is
also charged with planning for institutional-based SNF beds, it
also wasted over a decade with no planning to ensure an adequate
supply of SNF beds will be available in San Francisco to meet
the demand.
While the LTCCC is
also charged with planning for institutional-based SNF beds, it
also wasted over a decade with no planning to ensure an adequate
supply of SNF beds will be available in San Francisco to meet
the demand.
Out-of-County, Out of Mind
Health Commissioner David Pating’s hope to increase out-of-county and multi-county patient-dumping placements to deal with San Francisco’s so-called “post-acute care challenge,” is very troubling, given DPH’s own data.
 DPH has stalled this
reporter for over two years about providing an aggregate number
of out-of-county discharges from Laguna Honda Hospital, and only
in the past month has it provided a limited amount of data. Notably,
the Health Department and the Department of Aging and Adult Services
have shared the SF GetCare database for years, which contains
fields to track the discharge destination of either patients discharged
from LHH and SFGH, or patients who were “diverted” from
admission to LHH under a court-ordered Diversion and Community
Integration Program.
DPH has stalled this
reporter for over two years about providing an aggregate number
of out-of-county discharges from Laguna Honda Hospital, and only
in the past month has it provided a limited amount of data. Notably,
the Health Department and the Department of Aging and Adult Services
have shared the SF GetCare database for years, which contains
fields to track the discharge destination of either patients discharged
from LHH and SFGH, or patients who were “diverted” from
admission to LHH under a court-ordered Diversion and Community
Integration Program.
Common sense tells you that healthcare providers can’t do post-discharge patient follow-up to check on patient outcomes without knowing where patients are discharged to, and how to contact them for follow-up.
As Table 1 below shows, a minimum of 85 patients from LHH have been discharged out-of-county in the past three-and-a-half years, alone. The figure is thought to be far higher, but the Department of Public Health may be withholding release of the data for years prior to FY 2012–2013 for purely political reasons.
Table 1: Out-of-County Patient Discharges
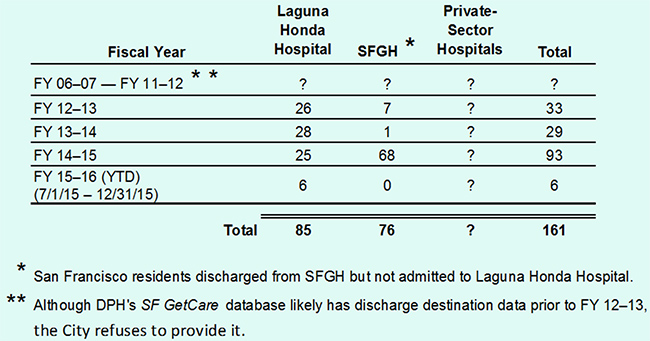
 Table 1 also shows
that across the same period of time, SFGH discharged another 76
San Franciscans to out-of-county Sub-Acute care, Skilled Nursing
Facility (SNF) care, Acute Rehab, and SNF Rehab facilities, bringing
the out-of-county discharge total between LHH and SFGH to 161,
with an unknown amount of out-of-county discharges by the two
facilities during the six fiscal years prior to FY 12–13
and also without an unknown amount of out-of-county discharges
made by private-sector hospitals.
Table 1 also shows
that across the same period of time, SFGH discharged another 76
San Franciscans to out-of-county Sub-Acute care, Skilled Nursing
Facility (SNF) care, Acute Rehab, and SNF Rehab facilities, bringing
the out-of-county discharge total between LHH and SFGH to 161,
with an unknown amount of out-of-county discharges by the two
facilities during the six fiscal years prior to FY 12–13
and also without an unknown amount of out-of-county discharges
made by private-sector hospitals.
LHH and SFGH operate only 1,172 beds of the estimated 5,483 total beds in acute care hospitals, and hospital-based- and freestanding-SNF facilities citywide, but no data is available on the number of out-of-county discharges made in the past three-and-a-half years in the remaining 4,311 citywide beds. So it is not known just how many additional out-of-county discharges there have been in addition to the 161 from LHH and SFGH that we know about.
Over the next 14 years, given a 1,745-bed SNF “supply” shortage and an additional 79,000 San Franciscans over the age of 65 driving “demand,” out-of-county discharges will likely soar.
Why didn’t DPH collect and report complete out-of-county discharge data for all San Francisco hospitals and SNF facilities in its “Framing San Francisco’s Post-Acute Care Shortage” report, a flawed analysis that may obscure the severity of un-met SNF needs?
Of note, although the February 16 “Framing San Francisco’s Post-Acute Care Shortage” report noted that many hospitals in San Francisco have had to increase the number of out-of-county discharges, private sector data is difficult to come by, perhaps due to risk management and public relations spin control. Reasonable people tend to believe that knowing just how many out-of-county discharges are actually being made could help inform planning efforts to protect elderly and disabled San Franciscans.
The report noted that on October 1, 2015, Laguna Honda Hospital reported that 11 people were on its wait list for long-term care, and 100 people were on San Francisco’s Jewish Home wait list for admission for long-term care. Couple that with data in the report that also noted that on October 21, 2015, of ten San Francisco acute-care hospitals surveyed — including SFGH — approximately 67 patients were waiting to be placed in a SNF, but didn’t note from which referring hospital, or to which SNF. That’s a lot of people who are experiencing un-met skilled nursing needs.
 There are plenty
of tiresome clichés bandied about in the “Framing
San Francisco’s Post-Acute Care Shortage” report.
Among the clichés is the sentence in the report that says:
There are plenty
of tiresome clichés bandied about in the “Framing
San Francisco’s Post-Acute Care Shortage” report.
Among the clichés is the sentence in the report that says:
This “reality” is driven, in part, by Health Commissioners such as David Pating who believes a solution is to increase the number of out-of-county discharges, apparently even if patients express a preference to remain in San Francisco. The “reality” is also driven by the utter lack of planning by San Francisco officials to have prevented this out-of-county patient dumping.
It’s increasingly painfully clear that San Francisco officials seem to prefer the excuse that there are “no beds at the inn,” an easy route to encourage — as Health Commissioner Pating appears to prefer — simply increasing the number of out-of-county discharges, rather than doing the hard work of planning for, and constructing, a sufficient number of post-acute and SNF facilities to keep San Franciscans housed in-county.
The Health Commission’s February 16, 2016 minutes show that for her part, Health Commissioner Cecila Chung — the only transgender woman to have served on San Francisco’s Health Commission — asked during the Health Commission’s meeting “whether San Francisco provides assistance to individuals re-entering the City after leaving [being discharged from] their out-of-county placements.”
 Neither Ms. Patil
nor any other official from the Department of Public Health provided
a direct answer to Commissioner Chung’s question. But it’s
an entirely relevant question that deserves an answer, since many
patients dumped out-of-county for short-term skilled nursing care
or rehabilitation may indeed want to return to our City, and not
be permanently disenfranchised and displaced out-of-county.
Neither Ms. Patil
nor any other official from the Department of Public Health provided
a direct answer to Commissioner Chung’s question. But it’s
an entirely relevant question that deserves an answer, since many
patients dumped out-of-county for short-term skilled nursing care
or rehabilitation may indeed want to return to our City, and not
be permanently disenfranchised and displaced out-of-county.
Chung’s question was astute, in part, because neither the City nor the Mayor’s Office of Housing and Community Development (MOHCD) has a preference priority in place for people discharged out-of-county to be eligible for either public-housing, or so-called “affordable housing,” to gain access to priority placement and return to San Francisco.
Once they’re discharged out-of-county, they are out of mind and are essentially handed a one-way ticket elsewhere, expected to never return.
And given that Health Commissioner Pating is aware of out-of-county patient discharges as far away as Los Angeles, what else does Pating know about the problem with no beds at the inn for San Francisco’s elderly and disabled who want to remain in-county during their final years?
 How much worse is
San Francisco’s long- and short-term care skilled nursing
bed shortage going to get, and how much longer will it go un-addressed?
Hasn’t 40 years of neglect in planning been long enough?
How much worse is
San Francisco’s long- and short-term care skilled nursing
bed shortage going to get, and how much longer will it go un-addressed?
Hasn’t 40 years of neglect in planning been long enough?
Monette-Shaw is an open-government accountability advocate, a patient advocate, and a member of California’s First Amendment Coalition. He received a James Madison Freedom of Information Award from the Society of Professional Journalists-Northern California Chapter in 2012. He can be contacted at monette-shaw@westsideobserver.
Postscript: “Dangerous Mix” in Califronia Nursing Homes
 After this article
was completed, the Sacramento Bee published an article on April 2 titled “Shifting
population in California nursing homes creates ’dangerous
mix’.” The article reported that the number of nursing
home residents under the age of 65 has surged 40% during the past
decade.
After this article
was completed, the Sacramento Bee published an article on April 2 titled “Shifting
population in California nursing homes creates ’dangerous
mix’.” The article reported that the number of nursing
home residents under the age of 65 has surged 40% during the past
decade.
The article notes the same statewide trend that San Francisco experienced at Laguna Honda Hospital with the disastrous “flow project,” in 2004 (or earlier) that placed a dangerous mix of younger, more able-bodied patients with behavioral issues at LHH to free up space at SFGH.
Westside Observer readers may recall that in March 2014, doctors Maria Rivero and Derek Kerr — both former senior physician specialists at LHH for over 20 years each — published their article, “Good-Bye Old Friends, Laguna Honda’s Changing Census” reporting that between 1999 and 2013 the number of patients at LHH over the age of 65 had plummeted from 67% to just 47%, and that the number of female patients had plunged from 56% to just 41% while at the same time the number of male patients soared from 44% to 59%. Rivero and Kerr astutely asked “What happens to ‘Old Friends’ who can no longer care for themselves? Where do they go? Who checks whether the care they receive elsewhere is comparable to what the new $585 million Laguna Honda provides?” They were concerned about volatile patient mixes.
The Bee’s article quoted Tippy Irwin, executive director of San Mateo County’s ombudsman services, as saying “The homes that we have known as havens for the frail elderly, as you can see, are no longer safe havens.”
 Instead, Irwin said,
many facilities now have what she described as a “dangerous
mix” — old, young, mentally ill, convicted felons, street
people in desperate need of care, and younger clients with chronic
illnesses, brain injuries and drug abuse problems.
Instead, Irwin said,
many facilities now have what she described as a “dangerous
mix” — old, young, mentally ill, convicted felons, street
people in desperate need of care, and younger clients with chronic
illnesses, brain injuries and drug abuse problems.
Industry leaders acknowledge the shifting demographics. Deborah Pacyna, spokeswoman for the California Association of Health Facilities, an industry trade group, said it “is an evolving issue and we continue to evaluate the impact on patient care.” The Bee reported Pacyna wrote in an e-mail: “Our first concern is the safety of our patients and staff,” and added “Our concern centers around a patient mix that places a frail elderly person in the same environment as a younger resident with mental illness or behavioral issues.”
Frances Salcedo, a longtime social services director at a suburban Los Angeles nursing home, said facilities aren’t always to blame for volatile patient mixes. Acute care hospitals sometimes fail to accurately or fully inform nursing homes about the mental health condition or behavioral issues of patients they refer, and a nursing home then may have a hard time discharging a difficult patient without facing penalties, she said.
A dangerous mix, indeed. And that is another reality, in addition to the new reality of simply being dumped out-of-county.