 Printer-friendly PDF file
Printer-friendly PDF fileJune 2020
COVID in Nursing Homes: A Geriatrician Worries About Mom
The City's COVID Curve Hasn’t Flattened
Printer-friendly PDF file
June 2020
COVID in Nursing Homes: A Geriatrician Worries About Mom
The City's COVID Curve Hasn’t Flattened
by Patrick Monette-Shaw
The wail “I can’t breathe” is heartbreaking. It haunts so many of us.
Berenice Palmer will soon celebrate her 103 birthday. One of her favorite quotes is from comedian and filmmaker Woody Allen:
“I don’t want to achieve immortality through my work.
I want to achieve it through not dying.”
For 102 years, Berenice has managed not to die, or die prematurely. She’s now a resident of a skilled nursing facility in San Francisco. Like Woody, Berenice doesn’t appear to be afraid to dying. She just doesn’t want to be there when it happens. A mom after my own heart!
Berenice’s daughter —Teresa Palmer, MD, a geriatrician — has grown worried. “I don’t want my mom to die,” says Dr. Palmer. She, along with several prominent healthcare organizations in California — including California Advocates for Nursing Home Reform (CANHR), the California Association of Health Facilities (CAHF), and the California Association of Long-Term Care Medicine (CALTCM) — are worried that placing COVID-19 patients in nursing homes that aren’t equipped to care for them, and also aren’t prepared to protect other nursing homes residents from acquiring the virus, is dangerous and may likely to lead to killing more older adults in nursing homes and assisted living facilities.
 “The lives of nursing home patients are worth something and they need to act like it,” Palmer says, with the “they” referring to both those who operate nursing homes, and state and local long-term care regulatory agencies. Palmer should know, since she was employed at San Francisco’s Laguna Honda Hospital and Rehabilitation Center for 15years, after starting there in 1989 and passing the Geriatric Medicine Certification exam in 1994 as a Board-certified geriatrician.
“The lives of nursing home patients are worth something and they need to act like it,” Palmer says, with the “they” referring to both those who operate nursing homes, and state and local long-term care regulatory agencies. Palmer should know, since she was employed at San Francisco’s Laguna Honda Hospital and Rehabilitation Center for 15years, after starting there in 1989 and passing the Geriatric Medicine Certification exam in 1994 as a Board-certified geriatrician.
Nursing Homes: Hotbeds
Although it is not widely reported in the news media, nursing homes are hotbeds for coronavirus outbreaks. To date, at least one-fifth of COVID-19 deaths nationwide are connected to nursing homes. One problem involves the lack of public information about just how many COVID-19 infections have occurred in nursing homes.
Unfortunately, many states — including California — are asking nursing homes to admit and take care of COVID-infected patients in their facilities, even if facilities aren’t equipped or prepared to do so safely.
Initially, the California Department of Public Health (CDPH) sent notices to each Skilled Nursing Facility (SNF) in the state indicating that the facilities might be required to accept COVID-19 patients, and should begin to prepare for admitting the patients — even if patients were still infectious.
Following sustained opposition from members of the public, CDPH loosened its requirements so that nursing homes could refuse to accept COVID-19 patients if the facilities are unable to follow Centers for Disease Control and Prevention (CDC) infection prevention and control procedures for the care of COVID-19 patients, including if facilities lack adequate personal protective equipment for workers; lack an ability to designate a specific wing, unit, or a separate building to isolate the COVID patients in; or lack other ways to prevent transmission of the coronavirus.
 It’s not known how many SNF’s notified CDPH that they would be unable to accept COVID-19 patients, and whether the State of California decided it had to look for alternate placement sites.
It’s not known how many SNF’s notified CDPH that they would be unable to accept COVID-19 patients, and whether the State of California decided it had to look for alternate placement sites.
As of May 1, California appeared to be so desperate to find facilities in which to place patients recovering from COVID-19 that the State began trying to entice assisted living facilities — which are licensed by the California Department of Social Services (CDSS), not the State’s Department of Public Health that licenses SNF’s — into accepting coronavirus patients by promising reimbursement of $1,000 per day per patient. Assisted living facilities that may not already be current hotbeds of COVID-19 transmission, but they may soon be.
Troublingly, pursuant to Governor Gavin Newsom’s emergency orders, CDSS has:
“… been granted the authority to waive any provisions of the Health and Safety Code or Welfare and Institutions Code, and accompanying regulations, interim licensing standards, or other written policies or procedures with respect to the use, licensing or approval of facilities or homes within CDSS’ jurisdiction in order to respond to the threat of COVID-19.”
It’s worrisome when any social services agency is granted authority to waive provisions of the health code and the institutions code that addresses licensing of medical and skilled nursing facilities, as if the COVID patients could be cared for by social workers rather than cared for by medical clinicians.
 Increasingly, the need for expanded public information about coronavirus cases and deaths in U.S. nursing homes and long-term care facilities has become greater, both because the public needs to know which specific facilities have problems and because governments need that information in order to direct resources to address the problems.
Increasingly, the need for expanded public information about coronavirus cases and deaths in U.S. nursing homes and long-term care facilities has become greater, both because the public needs to know which specific facilities have problems and because governments need that information in order to direct resources to address the problems.
As a reminder, look at what politicians are actually doing and what they have done, not what they’re saying. Governor Gavin Newsom and Mayor London Breed have talked a good game (what they’re saying) about expanding COVID-19 testing. But what have they actually done?
On April 16, President Trump boasted 3.5 million COVID-19 tests had been performed. Given a population of 350 million nationwide, that was a pathetic testing rate of just 1% of all Americans, nothing to be proud of — unless you’re Trump. [Aside: A month later, Trump bragged just 8 million COVID-19 tests had been performed by May 11, just 2.3% of all Americans. He didn’t mention that testing was largely restricted to only people displaying symptoms, not asymptomatic people, and he didn’t mention anything about national plans to implement on-going retesting.] It had taken until March 13 before Trump even got around to bothering to declare a National Emergency.
COVID-19 outbreaks in congregate settings around the world have left experts very worried. From jails to homeless centers, from skilled nursing facilities to nuclear-powered submarines, people who live in congregate settings face far greater risks of acquiring the virus.
On Tuesday, April 14 Governor Gavin Newsom outlined six key steps that need to need to be in place before he decides whether to “re-open” California and relax his statewide shelter-in-place order. The first two conditional steps involve 1) Greatly expanding COVID-19 testing capabilities and contact tracing; and 2) Maintaining protections for our most vulnerable living in congregate settings, particularly including seniors living in nursing homes and homeless people living unhoused or in shelters. National guidelines called for not re-opening until cases in a given jurisdiction have flattened and no deaths have occurred in the past 14-day period.
As of May 5, Newsom’s own first two criteria were nowhere near close to being achieved throughout California, let alone in San Francisco. Nor had San Francisco or California reached President Trump’s guidance that states could reopen when a state’s total coronavirus outbreak had no deaths during a 14-day period. No state had achieved Trump’s goal by May 5, and indeed California’s total cases continues to rise by 1,000 to 2,000 new cases per day.
Thankfully, Mayor London Breed did the right thing by extending her shelter-in-place order set to expire on May 3 through at least May 31, and didn’t let it expire. On May 13, the mayor of Los Angeles initially announced he would extend L.A.’s shelter-in-place order through the end of August. Breed may have to extend San Francisco’s stay-at-home order into June or July, or perhaps August.
Accelerators for COVID-19 Transmission: Nursing Homes
Nursing homes are considered by public health experts to be accelerators or incubators for the coronavirus, in part because of chronic understaffing, lax infection control procedures, and lax infection control enforcement; in part because social distancing is difficult in these facilities and other congregate settings; and in part because people with dementia’s have trouble adhering to physical- or social-distancing verbal queuing.
 Obviously, members of the public need to know which nursing homes have COVID-19 outbreaks in order to ask questions about what is being done to protect the residents, their families, and the community from further spread of the deadly virus. If for no other reason, facility-level COVID data should be disclosed so families can decide whether their relatives may want to move into, or move out of, any given facility.
Obviously, members of the public need to know which nursing homes have COVID-19 outbreaks in order to ask questions about what is being done to protect the residents, their families, and the community from further spread of the deadly virus. If for no other reason, facility-level COVID data should be disclosed so families can decide whether their relatives may want to move into, or move out of, any given facility.
Disturbingly, nursing homes, legislators at all levels of government, and regulatory agencies around the U.S. have failed to publicly release data in a timely manner — or at all — about the spread of, and prevalence and incidence of, COVID cases in nursing homes.
Not releasing facility-level COVID data leaves our democracy in the dark about what out government is doing to protect us. The secrecy behind which nursing homes have had COVID-19 outbreaks has impacted lives, and the thousands who have died. We deserve to see transparently what our government is doing — or isn’t doing — in our names.
Nursing Homes: Worldwide
 What do you do when you’re warned a worldwide pandemic is headed your way? If we want to save the most lives, don’t we need to focus on where the most lives are at risk revealed in other jurisdictions? The place where the most lives are going to be stolen by COVID-19 are the lives of people in nursing homes, assisted living facilities, and other long-term care facilities.
What do you do when you’re warned a worldwide pandemic is headed your way? If we want to save the most lives, don’t we need to focus on where the most lives are at risk revealed in other jurisdictions? The place where the most lives are going to be stolen by COVID-19 are the lives of people in nursing homes, assisted living facilities, and other long-term care facilities.
Sadly, the most lives stolen so far have been in nursing homes all over the world.
Statistics from additional countries mirror this global catastrophe.
Nursing Homes: United States
Unsurprisingly, it’s not just nursing homes in other countries. It was just as bad in the United States. Nursing homes should have been priority testing sites for COVID-19 nationwide, but weren’t despite the massive ten-fold surge in the number of U.S. nursing home deaths — from 2,246 to 28,100 deaths — during the one-month period ending May 11:
Figure 1: Massive Increase in Nationwide Nursing Home Deaths
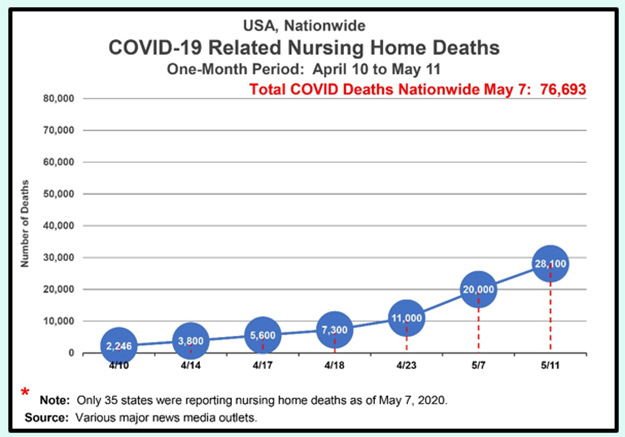
On April 10, NBC News reported there were 2,246 COVID-related deaths in nursing homes nationwide, which was likely vastly undercounted because of the lack of widespread testing and testing kits. The 2,246 deaths were only from 24 states, with large states like Florida, California, and Pennsylvania not reporting deaths from COVID in long-term care facilities. Many of the states reported patient deaths, but not deaths of nursing home staff.
 The New York Times published a story on April 14 that based on its research, 3,800 nursing home residents had died in U.S. The Times noted the 3,800 figure was likely an undercount since many facilities and states have declined to provide detailed information and data.
The New York Times published a story on April 14 that based on its research, 3,800 nursing home residents had died in U.S. The Times noted the 3,800 figure was likely an undercount since many facilities and states have declined to provide detailed information and data.
MSNBC’s Rachel Maddow reported on April 16 that the federal government was not tracking the number of COVID-19 cases in nursing homes nationwide. It seemed inconceivable that both the CDC (Centers for Medicare and Medicaid Services) and CMS (Centers for Medicare and Medicaid Services) were not tracking COVID cases as part of nursing home infection control regulators.
MSNBC reported on April 17 that there were more than 5,600 deaths at long-term care facilities across the U.S. The next day, news surfaced that nearly one-fifth of all COVID-19 deaths nationwide had occurred in nursing homes — 7,300 nursing homes deaths out of the then approximate 39,000 COVID deaths nationwide, or 19%. But that’s deceptive and probably widely under-reported, because only 19 states were reporting nursing home deaths from COVID as of April 18.
Five days later, Nightline reported that the number of COVID deaths in nursing home had reached 11,000 by April 23, 22% of the then 49,750 U.S. deaths. The April 23 Nightline report stated 26 states were reporting nursing home deaths — an increase of seven states — so its virtually certain that nursing home deaths are still being vastly under-reported, since just half of all states were reporting nursing home COVID data.
Over just one short month, the number of COVID-related deaths in U.S. nursing homes surged, when Rachel Maddow reported that there were at least 20,000 nursing home deaths nationwide as of May 7. Once again, that’s likely massively under-reported, since as Figure 1 shows only 35 states were reporting nursing home data at that point.
Maddow also reported on May 7 that accurate nationwide reporting of nursing home deaths may not become available until the end of May, if then. Maddow aired a segment on Vice President Mike Pence delivering Personal Protective Equipment (PPE) on behalf of the federal government for the first time since the COVID pandemic began to the Woodbine Rehabilitation and Healthcare Center, a nursing home in Alexandria, VA — without Pence wearing a face covering. Maddow reported that Seema Verma, Administrator of CMS who oversees nursing homes nationwide, accompanied Pence for the photo-op, also without wearing a face covering. (Pence, you may remember, also skipped wearing a face mask when he visited the Mayo Clinic in Rochester, Minnesota on April 28 after being informed that face masks were required by Mayo Clinic guidelines.)
Verma claimed CMS may begin releasing facility-level data on coronavirus cases and deaths in nursing homes around the country, perhaps at the end of May, after promising since mid-April that the data would soon be forthcoming. By the time we were scheduled to get that critical data perhaps by the end of May — assuming Verma wouldn’t delay releasing the data yet again — six to eight critical weeks would have slipped away.
Notably, President Trump nominated Verma to lead CMS on November 29, 2016 even before he took office; she was confirmed by the U.S. Senate on March 17, 2017. Trump expected Verma to take a hands-on role in his administration’s plans to repeal and replace President Barack Obama’s Affordable Care Act (ACA). Verma had previously been hired by then-Indiana Governor Mike Pence to develop Indiana’s Republican-friendly version of Medicaid expansion. The state paid her nearly $5 million over four years.
 Vice President Pence appointed Verma to the White House Coronavirus Task Force on March 2, 2020. Since then, Verma has stalled for over three months releasing accurate nationwide nursing home data. Ms. Verma appears to know where her bread is buttered, public health be damned. Which may explain her delay in releasing this critical nursing home data.
Vice President Pence appointed Verma to the White House Coronavirus Task Force on March 2, 2020. Since then, Verma has stalled for over three months releasing accurate nationwide nursing home data. Ms. Verma appears to know where her bread is buttered, public health be damned. Which may explain her delay in releasing this critical nursing home data.
President Trump’s Federal Nursing Homes Response
It was bad enough that President Trump and the federal government didn’t get around to distributing PPE to any nursing homes on behalf of the federal government until the first time on May 7, when Pence and Verma showed up without wearing facial coverings while delivering PPE supplies in Alexandria.
 Pence was scheduled to deliver more PPE to a yet-unnamed nursing home in Orlando, FL on Wednesday, May 20 as part of a belated White House propaganda initiative to deliver PPE to 15,000 nursing homes nationwide.
Pence was scheduled to deliver more PPE to a yet-unnamed nursing home in Orlando, FL on Wednesday, May 20 as part of a belated White House propaganda initiative to deliver PPE to 15,000 nursing homes nationwide.
On May 11, the Associated Press reported the White House had finally recommended all nursing home residents and staff be tested for COVID-19 within two weeks. Vice President Mike Pence, who heads the White House Coronavirus Task Force, told governors during a conference call the federal government’s recommendation was nursing home testing be done.
The AP reported that Dr. Deborah Birx, coordinator of the White House Coronavirus Task Force, also told governors on May 11 to focus over the next two weeks on testing all one million nursing home residents nationwide. Birx has been the U.S. Global AIDS Coordinator since 2014.
Brix made no mention of how over one million tests would be administered in a 14-day period. And she said nothing about follow-up re-testing plans going forward.
Trump and Verma also asserted on May 12 that testing of nursing home patients and staff should be done within two weeks. There’s no word yet on whether that actually happened.
The Trump administration’s belated focus on nursing home testing stands in stark contrast to New York Governor Andrew Cuomo, who had announced the day before on May 10 a new executive order containing several new rules, including:
To drive home his point about the urgency of the nursing home testing, Cuomo stated the same day that nursing homes and adult care facilities that violate his new rules could have their operating licenses suspended or revoked, and could face non-compliance penalties of $2,000 per day.
Cuomo stands in stark contrast to President Trump. Despite Trump’s pitch with Verma on May 12 calling for increased testing in nursing homes, on May 14 Trump made an about-face, asserting:
“It could be that testing is over-rated. If we didn’t do any testing, we would have very few [COVID] cases.”
— Donald J. Trump
May 14, 2020
That may be part and parcel of Trump’s hopes to review all COVID-19 deaths to see if they were misclassified, hoping to reduce the sheer raw number of COVID fatalities. What Trump seems incapable of understanding, as Maddow noted, is that even without testing you’d likely still have the same number of cases and deaths (if not many more, due to missed opportunities to do contact tracing), but you just wouldn’t know about them (or know where to direct resources).
 Part of Trump’s problem is that he just doesn’t get it that by changing data and restricting release of information about just how bad things are doesn’t actually change just how bad things are in reality land. He may figure that he can just stop telling us information, but that’s not going to stop us from wanting the information. We just want to be told the truth.
Part of Trump’s problem is that he just doesn’t get it that by changing data and restricting release of information about just how bad things are doesn’t actually change just how bad things are in reality land. He may figure that he can just stop telling us information, but that’s not going to stop us from wanting the information. We just want to be told the truth.
Is this Trump’s newest ostrich-with-his-head-in-the-sand nincompoopism? Oh, wait! I forgot this is Trump we’re talking about:
“[Trump] was the dumbest goddamn student I ever had.”
— William T. Kelley, Professor
Wharton Business School
State-Specific Nursing Home Data
News reports on April 17 indicated that 40% of COVID-19 cases in New Jersey and 50% of cases in Massachusetts were residents of nursing homes. Just days before, Massachusetts Governor Charles Baker had reported on April 13 that of 800 positive nursing home cases in his state, 46% (≈368 people) occurred in nursing homes. Within four days, the percentage of infections in Massachusetts nursing homes on April 17 had climbed significantly.
On April 19, New York State reported that 25% of the COVID deaths in the state had occurred in nursing homes. The day before, it was reported 1,200 of California’s COVID cases had occurred in nursing homes, a number that appeared to be vastly under-reported.
As of April 30, the Rachel Maddow Show reported several states have been particularly hard hit with nursing home deaths:
Notably, Maddow didn’t include summaries of California and New York State nursing home deaths data.
The April 11 New York Times article noted that the number of nursing home residents and employees who had died at that point accounted for more than half of all deaths in 14 states.
In Kirkland, Washington the coronavirus outbreak at the Life Care and Rehabilitation Center nursing home initially reported 15 patients had died, but that quickly grew to 37 patient deaths and resulted in a $611,000 fine on April 2 from the Centers for Medicare and Medicaid (Medi-Cal) Services (CMS) for the nursing homes’ failure to report the increasing rate of respiratory infections. News has since surfaced that in addition to the CMS fine, the family of a patient who died at the facility has filed a wrongful death lawsuit.
 Within a month — and before the end of May when nursing homes were required to respond to the new testing guidance CMS and CDC had mandated — the incidence of COVID-related deaths in nursing homes nationwide grew even worse.
Within a month — and before the end of May when nursing homes were required to respond to the new testing guidance CMS and CDC had mandated — the incidence of COVID-related deaths in nursing homes nationwide grew even worse.
On May 26 Forbes published an article noting that by that point there were still seven states that refuse to report COVID-related deaths in nursing home and long-term care facilities, including Hawaii, New Mexico, North Dakota, South Dakota, Missouri, Michigan, and Vermont. The federal government had instituted such a requirement on May 5 requiring reporting of COVID-related nursing home deaths.
Map 1: 42% of COVID Deaths From 0.62% Of U.S. Population
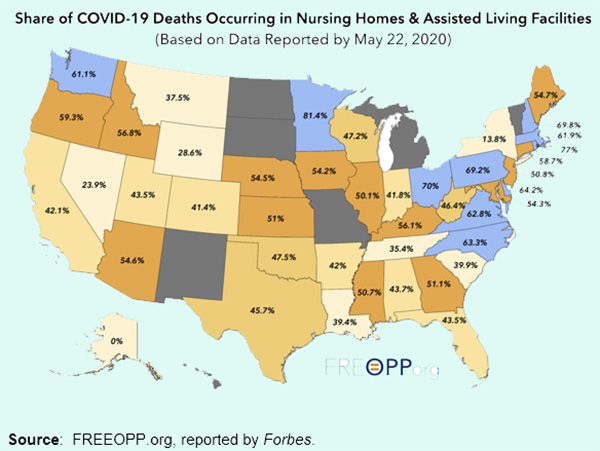
Forbes reported that “Among states reporting their death totals, 42% of COVID deaths have taken place in long-term care facilities,” and added “Let that sink in: 42% of all COVID-19 deaths are taking place in facilities that house 0.62% of the U.S. population.”
 Forbes noted the 42% is likely an undercount, because other states — including New York, the epicenter of COVID-19 in the U.S. with 30,565 COVID-related deaths as of June 13 — exclude from their nursing home death tallies those who died in a hospital, even if they were originally infected in a long-term care facility. Add in nursing home residents who died in hospitals in the remaining seven states, and it’s more likely that 50% of COVID-related deaths nationwide have occurred among nursing homes.
Forbes noted the 42% is likely an undercount, because other states — including New York, the epicenter of COVID-19 in the U.S. with 30,565 COVID-related deaths as of June 13 — exclude from their nursing home death tallies those who died in a hospital, even if they were originally infected in a long-term care facility. Add in nursing home residents who died in hospitals in the remaining seven states, and it’s more likely that 50% of COVID-related deaths nationwide have occurred among nursing homes.
Figure 1 shows, among other things:
Also troublingly, CMS and CDC do not appear to be requiring nursing facilities in five U.S. territories (American Samoa, Guam, the Northern Mariana Islands, Puerto Rico, and the U.S. Virgin Islands) report COVID-19 case data and deaths. So, the impact on Americans living in those territories is not uniformly reported and may push total U.S. cases far higher.
California Nursing Homes: Beset by Sketchy Data
On March 30 and April 1, 2020 California’s Department of Public Health (CDPH) issued a directive to all skilled nursing facilities in California stating that all SNF’s should prepare to accept COVID-19 patients. CDPH’s directives stated SNF’s shall not refuse to admit or readmit a resident based on their status as a suspected or confirmed COVID-19 case: “SNF’s shall institute appropriate precautions to prevent the spread of infection to health care personnel and  other residents.”
other residents.”
Multiple patient advocacy groups promptly objected to CDPH’s directives.
The California Association of Health Facilities (CAHF) issued a statement before April 15 saying it doesn’t support the placement of COVID-19 positive patients in skilled nursing facilities. CAHF believed doing so would only be acceptable if a facility has a separate wing or building to place COVID patients in; if a facility has adequate staffing, proper and sufficient equipment; and if a facility fully adheres to infection control guidelines.
For its part, California Advocates for Nursing Home Reform (CANHR) issued an emergency action plan on April 10 arguing that facilities without any patients with COVID should refuse to admit infectious COVID-19 patients, and recommended that specific facilities be established and dedicated to accepting patients being discharged from acute-care hospitals.
CANHR recommended establishing COVID-19-only dedicated post-acute care facilities in counties and require all hospital post-discharge patients to be tested for COVID-19 and if positive, transferred to such facilities.
CANHR recommended the CDPH directives be revised to prohibit SNF’s from admitting COVID-19 patients from hospitals and to prohibit hospitals from sending them, in part because too many SNF’s have proven they cannot handle the COVID-19 virus and it will be a death knell for the residents. CANHR believed California should also immediately prohibit all inter-facility transfers, unless they are to COVID-19-only dedicated post-acute care facilities.
CAHNR also noted the California Association of Long-Term Care Medicine (CALTCM) had developed a detailed plan for the establishment of COVID-19 only facilities that the State of California should adopt.
 Oddly, on April 12, one news source presented a list of 21 states across the U.S. with the highest numbers of positive tests performed per 100,000 of the population. Sadly, California didn’t even make the list. Six days later, on April 18, another news source reported California ranked #48 in the number of COVID-19 tests performed to date. Newsom talked a great game, but statewide testing was pathetic at that point, mostly because of the difficulty in acquiring the test kits, reagents, swabs, etc., and because of a backlog in testing capacity at private and public laboratories.
Oddly, on April 12, one news source presented a list of 21 states across the U.S. with the highest numbers of positive tests performed per 100,000 of the population. Sadly, California didn’t even make the list. Six days later, on April 18, another news source reported California ranked #48 in the number of COVID-19 tests performed to date. Newsom talked a great game, but statewide testing was pathetic at that point, mostly because of the difficulty in acquiring the test kits, reagents, swabs, etc., and because of a backlog in testing capacity at private and public laboratories.
Since April 12, COVID cases in California nursing homes worsened. As of May 5, 47% to 50% of COVID-19-related deaths in California had occurred in nursing homes and assisted living facilities. [It’s grown, since.]
After New York’s governor Andrew Cuomo announced on April 23 that he was requiring New York State facilities to provide public data about the number of COVID cases in New York nursing homes, California’s Department of Public Health (CDPH) finally released preliminary data about the number of COVID-19 cases in California nursing homes on Friday, April 17 reporting that 258 of California’s 1,224 nursing homes had reported one or more COVID cases among staff or residents.
CDPH’s inaugural April 17 report indicated 1,279 staff and 1,721 residents had tested positive in California SNF’s as of April 17, 2020 — for a total of 3,000 positive cases. [Those numbers grew to 5,702 staff and 9,718 residents, for a total of 15,420 cases just in California SNF’s by May 31, excluding assisted living facilities — a 414% percent change increase across only six weeks.]
 California’s initial data didn’t include deaths or exact figures reporting the number of infected patients and staff at most of the skilled nursing facilities. The data was also limited to Skilled Nursing Facilities (SNF’s) licensed by CDPH and didn’t include assisted living facilities, Residential Care Facilities for the Elderly (RCFE’s), Adult Rehabilitation Facilities (ARF’s), or board-and-care homes, all of which are licensed by other California state agencies, not CDPH.
California’s initial data didn’t include deaths or exact figures reporting the number of infected patients and staff at most of the skilled nursing facilities. The data was also limited to Skilled Nursing Facilities (SNF’s) licensed by CDPH and didn’t include assisted living facilities, Residential Care Facilities for the Elderly (RCFE’s), Adult Rehabilitation Facilities (ARF’s), or board-and-care homes, all of which are licensed by other California state agencies, not CDPH.
Unfortunately, CDPH’s data was deeply flawed then, and still is.
First, CDPH had to release an update to its data the very next day on April 18 to remove three facilities that had initially been wrongly named as having COVID cases. By April 24, CDPH was shamed into reporting limited data listing all 1,224 nursing homes in the State, not just the first 258 facilities named on April 17.
Second, the data was a one-time “point-in-time” snapshot; it wasn’t known whether CDPH would update the on-line regularly, or how often.
Third, the data was deeply flawed because for both staff infections and patient infections, CDPH only reported whether a given facility had less than 11 cases among either staff or patients, and didn’t report the number of actual cases in each facility, under the pretext of protecting patient and staff medical records privacy.
For instance, CDPH’s reported there were less than 11 staff members at San Francisco’s Laguna Honda Hospital who had tested positive for COVID-19, but local news media reported that San Francisco’s Department of Public Health confirmed on April 16 that 15 LHH staff members had tested positive. Similarly, CDPH reported zero patient infections at LHH — not merely “less than 11” — despite the fact that SFDPH had reported four patients had tested COVID-19 positive as early April 6.
CDPH also reported on April 17 that the Central Gardens SNF in San Francisco had 26 staff members and 36 patients who had tested COVID-positive. But media reports show 28 staff members and 39 residents at Central Gardens on Ellis Street in the Western Addition neighborhood have tested positive, including four patients who have died.
The CDPH report listed just one facility in Costa Contra County at the Orinda Care Center, LLC — despite the fact that Contra County officials have released public data showing 14 skilled nursing facilities in the county have reported staff or patient COVID-19 infections.
Some time before April 8, news broke reporting 60 cases of COVID among staff and residents of Gateway Care and Rehabilitation Center in Hayward (Alameda County), including 10 patient deaths. By April 15, the viral outbreak had grown to 65 infections and had claimed 13 lives, and by April 17 CDPH reported a total of 102 cases at Gateway Care (33 staff and 69 residents). By April 15, the Gateway outbreak had spread to a neighboring facility, Windsor Post-Acute Care Center, infecting another 10 staff plus another 7 residents. [Strangely, as of June 3 CDPH reduced the Gateway Care cumulative data downward to 31 staff and 48 residents, but it’s not clear why the total cases dropped from 102 to 79.]
CDPH initially said on April 17 that in the future it planned to begin reporting the number of patient deaths at each SNF, but how soon CDPH would begin reporting data on staff and patient deaths at each facility also wasn’t initially announced or known. At some point, CDPH started reporting the number of staff and patient deaths in each facility, but only on-line. As of May 1, when site visitors download the Excel file reporting data for each facility, only the number of staff and patient infections are reported in the downloaded file; for some reason, the data shown on-line reporting the number of patient and staff deaths were not included in the downloaded file.
 On May 6 CDPH finally started including facility-level staff and resident deaths in the downloaded Excel files, without any explanation of why it had suddenly started reporting deaths at specifically-named SNF’s. What was that delay all about?
On May 6 CDPH finally started including facility-level staff and resident deaths in the downloaded Excel files, without any explanation of why it had suddenly started reporting deaths at specifically-named SNF’s. What was that delay all about?
One glaring problem with the CDPH data is that as of May 13, only 85% of California’s 1,224 SNF’s had complied with reporting COVID-19 data to the State. Fully 15% of the SNF’s — 184 facilities — apparently believed they didn’t have to comply with reporting the data to CDPH, so the data presented was obviously woefully incomplete and flawed. Why hadn’t CDPH — or the State legislature — gotten involved to require the errant 184 SNF’s to report their data?
Another problem with the delay in reporting is that patients and their families have no idea of which of the facilities may be placing them and their loved ones at risk. Another problem with the delayed reporting is that legislators around the state have no idea of where the hot spots are in nursing facilities throughout the state.
Does CDPH really believe it can pass off this bogus “data,” after local Health Departments and local media have been reporting data that clearly exceeds what CDPH is willing to report officially? How dumb does CDPH think we are?
What About Other California Facilities?
In addition to the 1,224 SNF’s licensed by CDPH, there are approximately 7,400 other facilities in California licensed to provide lower levels of care for people who don’t qualify for 24/7 skilled nursing level of care, including Residential Care Facilities for the Elderly (RCFE’s), Adult Residential Facilities (ARF’s), and smaller so-called “board-and-care” homes. The three other types of facilities are often smaller facilities, many having just six to ten patients.
 A week after CDPH began reporting on-line updates of the number of patients and staff who tested positive for COVID-19 in the state’s SNF’s on April 17, California’s Department of Social Services (CDSS) belatedly also began >reporting1 the number of patients and staff who had tested positive in RCFE’s and ARF’s on April 22. Weirdly, CDSS lumps both patient and staff infection data into a single number, and also lumps both the RCFE and ARF data into the same single number. Why can’t CDSS stratify the data into four numbers, so we know how many patient vs. staff infections have occurred in each of the two types of facilities?
A week after CDPH began reporting on-line updates of the number of patients and staff who tested positive for COVID-19 in the state’s SNF’s on April 17, California’s Department of Social Services (CDSS) belatedly also began >reporting1 the number of patients and staff who had tested positive in RCFE’s and ARF’s on April 22. Weirdly, CDSS lumps both patient and staff infection data into a single number, and also lumps both the RCFE and ARF data into the same single number. Why can’t CDSS stratify the data into four numbers, so we know how many patient vs. staff infections have occurred in each of the two types of facilities?
The number of COVID infections in California skilled nursing and assisted living facilities is worse than currently reported in the national news media.
Table 1: COVID in California Skilled Nursing and Assisted Living Facilities
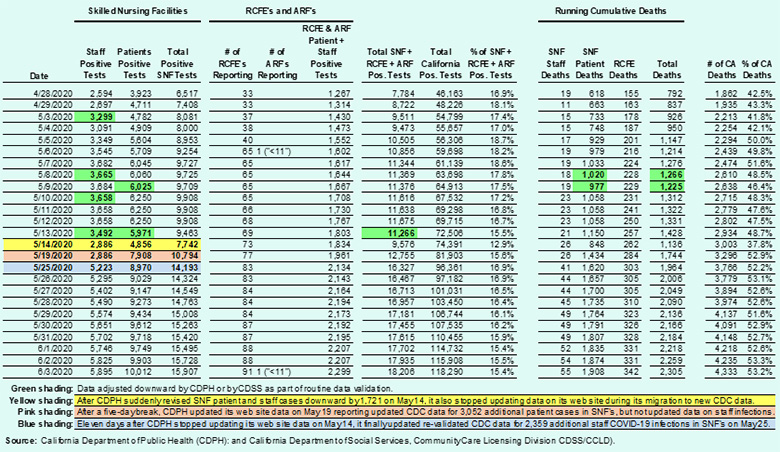
 Table 1 illustrates that as of June 3, 2020 fully 53% of California’s COVID cases had occurred in skilled nursing and assisted living facilities, but that’s probably an undercount for a number of number of reasons:
Table 1 illustrates that as of June 3, 2020 fully 53% of California’s COVID cases had occurred in skilled nursing and assisted living facilities, but that’s probably an undercount for a number of number of reasons:
 Since CDPH is still “scrubbing” data by hiding facility-level data behind de-identification guidelines (using reporting of “<11”) to protect HIPAA patient-specific data, its unclear whether accurate cumulative data is being under-reported.
Since CDPH is still “scrubbing” data by hiding facility-level data behind de-identification guidelines (using reporting of “<11”) to protect HIPAA patient-specific data, its unclear whether accurate cumulative data is being under-reported.On June 15, Governor Newsom held a televised press briefing for the first time in some days, during which he observed that of the then 5,000-plus COVID-19-related deaths in California, 50.3% had occurred in nursing facilities across the state.
CDPH: Better Late Than Never
The California Department of Public Health (CDPH) hasn’t been behind the eight ball during much of the COVID-19 pandemic. CDPH routinely issues guidance to licensed healthcare facilities through its All Facilities Letters (AFL). On May 11, CDPH issued AFL #20-52 requiring all skilled nursing facilities in the state to expand their existing infection control policies by developing and implementing CDPH-approved COVID-19 mitigation plans for their facility within 21 calendar days.
Eleven days later CDPH issued AFL #20-53 on May 22, which only recommended (but didn’t explicitly require) each SNF in the state develop COVID-19 Mitigation Plans that include baseline, surveillance, and response-driven testing of SNF residents and healthcare staff to prevent spread of COVID-19 infections.
But sadly, it took CDPH until June 2 before it got around to issuing AFL #20-55, which requires that all SNF’s in the state perform and report to CDPH the results of COVID-19 baseline testing of all residents and healthcare staff in facilities that did not currently have any positive cases, and that the baseline testing be completed by June 30, 2020.
The three delays were ridiculous:
 By May 22, when CDPH merely recommended developing mitigation plans in SNF’s, California had 3,649 COVID-19 deaths, of which 1,760 (48.2%) had occurred in SNF’s or RCFE’s, and deaths nationwide had reached 97,490. CDPH must have known this data on May 22.
By May 22, when CDPH merely recommended developing mitigation plans in SNF’s, California had 3,649 COVID-19 deaths, of which 1,760 (48.2%) had occurred in SNF’s or RCFE’s, and deaths nationwide had reached 97,490. CDPH must have known this data on May 22.It’s almost as if CDPH believed ignorance is bliss when it comes to completing baseline testing.
That it took CDPH until June 2 to mandate baseline testing be completed by the end of June was all the more shocking because two months earlier Governor Newsom pledged on April 10 he would make addressing the threat of COVID in nursing homes his top priority. At this point, every day of needless delay completing baseline testing matters.
 It was also shocking because CMS Administrator Verma had asserted a month earlier on May 12 that COVID testing of nursing home patients and staff nationwide should be done within two weeks. Why CDPH extended Verma’s end-of-May directive for baseline testing until the end of June wasn’t explained.
It was also shocking because CMS Administrator Verma had asserted a month earlier on May 12 that COVID testing of nursing home patients and staff nationwide should be done within two weeks. Why CDPH extended Verma’s end-of-May directive for baseline testing until the end of June wasn’t explained.
I guess better late than never may be better, but how many deaths may have been avoided had earlier is better been used? After all, those lives lost were not disposable, since those lives matter, too.
Data from the state also remains sketchy because of the spotty — or complete lack of — reporting by some facilities, delays in reporting by many facilities, and the failure to provide full data by hiding behind HIPAA patient privacy protections to withhold data that can easily be aggregated without violating individual patient privacy.
Testing San Francisco’s 21 SNF’s, Including Laguna Honmda Hospital
On April 13, San Francisco’s Director of Public Health, Grant Colfax reported that 303 of LHH’s approximately 1,700-member staff had been tested for COVID by either DPH or by staff members’ own medical providers. That meant just 17.8% of LHH’s staff had been tested by April 13. Similarly, Colfax announced 215 of LHH’s 750 residents had been tested, which represented just 27.6% of patients had been tested. [It took another six weeks into early June before all LHH staff and residents completed the initial round of universal testing.]
On April 22, Dr. Colfax indicated San Francisco has an aspirational goal of providing universal access to COVID-19 testing. The City was nowhere near close to being able to provide universal testing for people who have symptoms, let alone those who may have been infected but had remained asymptomatic.
The City began testing a limited number of asymptomatic “essential” employees on May 4, but as of May 19 San Francisco was still predominantly testing only those exhibiting coronavirus symptoms. Universal testing of all asymptomatic San Franciscans has not begun.
 On May 1, San Francisco health officials announced the City would mandate regular, universal COVID-19 testing for residents and staff in all of the City’s 21 public and private skilled nursing facilities. Testing was to begin Monday, May 4 at Laguna Honda Hospital, but for some reason was delayed and didn’t get underway until Wednesday, May 6. It was expected testing at LHH would be completed by Friday, May 8, but as of May 19 testing of all of LHH’s staff had not yet been completed. This clearly took much longer than the initial plan.
On May 1, San Francisco health officials announced the City would mandate regular, universal COVID-19 testing for residents and staff in all of the City’s 21 public and private skilled nursing facilities. Testing was to begin Monday, May 4 at Laguna Honda Hospital, but for some reason was delayed and didn’t get underway until Wednesday, May 6. It was expected testing at LHH would be completed by Friday, May 8, but as of May 19 testing of all of LHH’s staff had not yet been completed. This clearly took much longer than the initial plan.
The initial announcement on May 1 indicated San Francisco would “for the most part” supply the test kits for the first round of testing, presumably in all 21 SNF facilities. But that came with a caveat: “As the process matures and skilled nursing facilities start doing their own testing, they may be responsible for [acquiring] the kits [perhaps at their own expenses], as well, when they have adequate supply,” Department of Public Health spokesperson Rachel Kagan said.
Testing of all 21 SNF’s was projected to take roughly a month, but three weeks into May only half of the facilities had completed testing. The Jewish Home said its full staff and patients would be tested between May 21 and May 25 but expected results wouldn’t be announced until June 1.
 During Breed’s press conference on May 19, San Francisco Director of Public Health Grant Colfax presented an update on “universal testing” in all of the City SNF’s. Colfax said testing of 2,087 people — 718 patients and 1,369 staff — had been completed at LHH. Colfax said the rest of LHH’s staff would finish testing by the next week, but didn’t explicitly mention 400 of LHH’s staff apparently remained to be tested. Turned out, it took over two weeks, not one, to complete that testing.
During Breed’s press conference on May 19, San Francisco Director of Public Health Grant Colfax presented an update on “universal testing” in all of the City SNF’s. Colfax said testing of 2,087 people — 718 patients and 1,369 staff — had been completed at LHH. Colfax said the rest of LHH’s staff would finish testing by the next week, but didn’t explicitly mention 400 of LHH’s staff apparently remained to be tested. Turned out, it took over two weeks, not one, to complete that testing.
Colfax noted that as a result of the expanded testing at LHH, four new cases were discovered that lead to uncovering four more cases. The cumulative count rose to 29 cases at LHH (11 residents and 18 staff), an increase of eight cases since the previous report on April 26 when 5 residents and 16 staff COVID cases were reported.
The five initial patient cases at LHH were in the South 4 and South 5 neighborhoods. Among the additional six patient cases, five occurred on South 2, and one on North 4. The six new patient cases on North 4 and South 2 were worrisome, because they were in different areas of the hospital, with the North Tower almost being a separate building.
Let’s review the timeline: On March 6, Breed closed LHH to all visitors. Eighteen days later, on March 24 five LHH staff members were reported to have tested positive; the next day, LHH’s first patient tested positive.
 Those first six cases so alarmed Breed that she brazenly wrote to Robert Kadlec, the U.S. Department of Health and Human Services Assistant Secretary for Preparedness on March 27, requesting 110 federal staff be sent to San Francisco to slow the spread of COVID-19 in the City, particularly at Laguna Honda Hospital. At that point, there were just 7 COVID cases (6 staff and 1 resident) at LHH.
Those first six cases so alarmed Breed that she brazenly wrote to Robert Kadlec, the U.S. Department of Health and Human Services Assistant Secretary for Preparedness on March 27, requesting 110 federal staff be sent to San Francisco to slow the spread of COVID-19 in the City, particularly at Laguna Honda Hospital. At that point, there were just 7 COVID cases (6 staff and 1 resident) at LHH.
The first question was, did the U.S. DHHS have 110 extra staff sitting around it could dispatch to a single city? After all, there are approximately 15 additional U.S. cities with populations roughly the size of San Francisco. Where were the feds supposed to come up with that level of staffing — 1,760 federal employees — to support sending 110 staff to each of the 16 cities needing help, with Trump sitting in the White House?
 Three days later, Breed posted a press release on March 30 in which she indicated LHH had 11 COVID infections — 9 staff and 2 residents. She also indicated on March 30 that six federal and state experts — not 110 — had arrived to help. Her press release indicated she was still “awaiting a response” from Secretary Kadlec.
Three days later, Breed posted a press release on March 30 in which she indicated LHH had 11 COVID infections — 9 staff and 2 residents. She also indicated on March 30 that six federal and state experts — not 110 — had arrived to help. Her press release indicated she was still “awaiting a response” from Secretary Kadlec.
In response to a records request placed on June 7 seeking any response to Breed from Kadlec or the U.S. DHHS, the Mayor’s office responded on June 9 saying it had “conducted a search for any written response from DHHS and found none [no response from DHHS]. Accordingly, we have no records to provide in response.”
It’s hard to believe that Kadlec or his office did not respond in writing to Breed offering a written explanation or justification so it would be on the public record. I guess that means Breed may have gotten six, but not 110, federal helpers.
A month after Breed went seeking federal support, staff infections at LHH had risen to 16 and patient infections had risen to 5, for a total of 21 cases by April 27, despite the handful of federal and state assistance.
 Three weeks later, COVID infections at LHH rose to 29 cases by May 19 — 18 among staff and 11 among residents. That was at least six weeks after infection control specialists from the CDC and state were ostensibly brought in to stop the LHH COVID outbreak from growing further.
Three weeks later, COVID infections at LHH rose to 29 cases by May 19 — 18 among staff and 11 among residents. That was at least six weeks after infection control specialists from the CDC and state were ostensibly brought in to stop the LHH COVID outbreak from growing further.
On May 19 Colfax said testing in the 21 SNF’s in the City was on-going, and 40% of testing of staff and patients was completed, with five facilities finished, four underway, and the remaining 10 or 11 facilities were still being “planned.” He didn’t name the names of any of the other facilities.
Two weeks later, only 17 of San Francisco’s 21 SNF’s had completed testing as of June 1. Slide 9 in a DPH presentation informed the Health Commission on June 2 that only 17 of the facilities had completed the “universal” testing.
A records request was submitted to DPH on June 4 seeking 1) A list of the names of the 17 facilities in which testing had concluded by June 1 and data on the number of positive infections of staff and residents in each facility; and 2) The names of the 4 remaining SNF’s that were still undergoing universal baseline testing of all staff and residents.
Sadly, DPH declined to provide any records, saying on June 5 “The San Francisco Dept. of Public Health does not have responsive records at this time. We are committed to protecting the privacy and confidentiality of patients.”
 This far into the pandemic, why is SFDPH not even willing to release the names of the 17 facilities that completed universal COVID-testing by June 1? Releasing the names of those facilities can not possibly involve HIPAA patient privacy protection violations.
This far into the pandemic, why is SFDPH not even willing to release the names of the 17 facilities that completed universal COVID-testing by June 1? Releasing the names of those facilities can not possibly involve HIPAA patient privacy protection violations.
It took until June 18, when CMS provided an update on its web site that we learned that as of June 7, LHH COVID cases had reached 71 — 46 staff and 25 residents — fully 10 times more than Breed reported on March 27 as 7 total cases at LHH. We didn’t learn of that ten-fold increase in cases at LHH from Breed or Colfax. We learned of it from CMS public data.
Breed Admits “We Haven’t Lowered the Curve”
“The numbers are still going up. The number of deaths are still going up. We have not lowered the curve.”
— London Breed, Mayor
May 6, 2020
Data posted on the San Francisco Department of Public Health’s COVID-19 Tracker web site documented that on May 6, our City had 1,806 COVID-19-positive cases, and a total of 33 deaths from the coronavirus. In the 19 calendar days since May 6, the COVID-19 Tracker web site reported:
Figure 2: COVID Curve Is Not Flattening
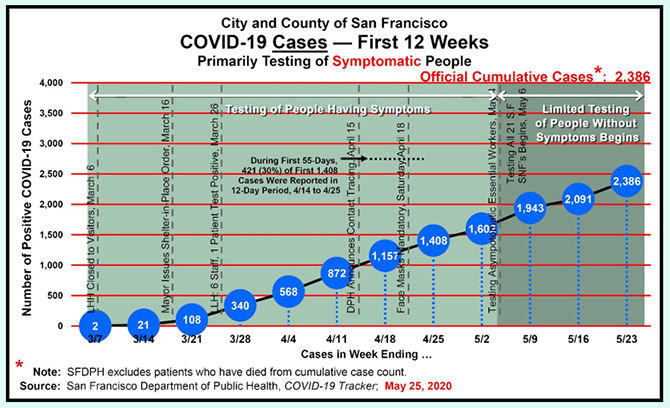
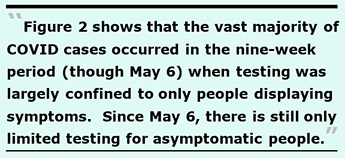 Figure 2 shows that the vast majority of COVID cases occurred in the nine-week period (though May 6) when testing was largely confined to only people displaying symptoms. Since May 6, there is still only limited testing for asymptomatic people, and the total number of cases are still going up. DPH had not finished testing all residents and staff in all 21 San Francisco skilled nursing facilities that were scheduled to complete testing before the end of May, as had been promised.
Figure 2 shows that the vast majority of COVID cases occurred in the nine-week period (though May 6) when testing was largely confined to only people displaying symptoms. Since May 6, there is still only limited testing for asymptomatic people, and the total number of cases are still going up. DPH had not finished testing all residents and staff in all 21 San Francisco skilled nursing facilities that were scheduled to complete testing before the end of May, as had been promised.
Figure 3: Weekly COVID Cases
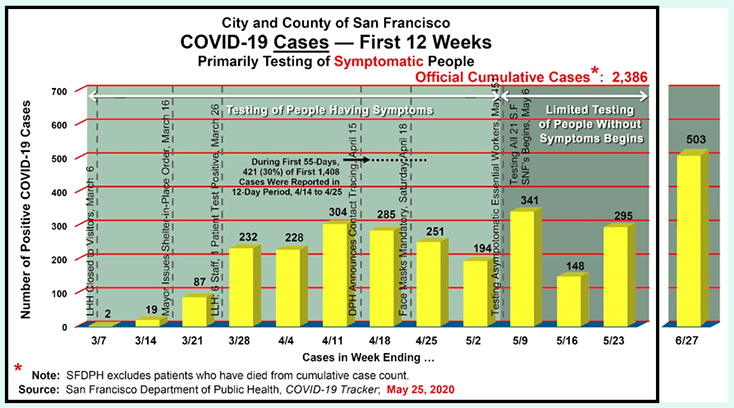
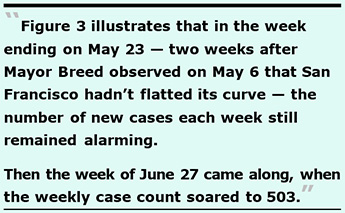
Figure 3 illustrates that in the week ending on May 23 — two weeks after Mayor Breed observed on May 6 that San Francisco hadn’t flatted its curve — the number of new cases each week still remained alarming. Indeed, May 23 (the 12th week of reporting) was the third highest week in weekly cases (341 cases ending the week May 9, 304 cases ending the week of April 11, and then 295 cases in the week ending May 23).
Then came the week ending June 27, when weekly cases soared to 503.
Figure 4: Cumulative Testing
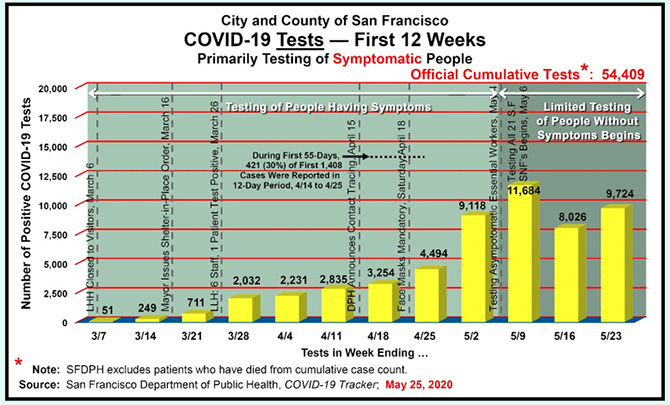
 Figure 4 illustrates that fully 29,434 — 54% — of San Francisco’s 54,409 tests conducted through May 23 were taken during the three weeks ending May 9, May 16, and May 23 after Breed admitted on May 6 that San Francisco’s curve had not been flattened. That’s because testing was still largely restricted to only essential workers who may be asymptomatic, not all vulnerable populations who may also be asymptomatic.
Figure 4 illustrates that fully 29,434 — 54% — of San Francisco’s 54,409 tests conducted through May 23 were taken during the three weeks ending May 9, May 16, and May 23 after Breed admitted on May 6 that San Francisco’s curve had not been flattened. That’s because testing was still largely restricted to only essential workers who may be asymptomatic, not all vulnerable populations who may also be asymptomatic.
When is the City going to mandate — and rapidly conduct — testing of all staff and residents in Residential Care Facilities for the Elderly (RCFE’s), Adult Residential Facilities (ARF’S), and all other assisted living facilities in the City, in addition to universal testing in all of the 21 SNF’s? So far, Breed, Colfax and San Francisco haven’t indicated when the City will start or even complete universal testing in other assisted living congregate facilities. Every day of delayed universal baseline testing matters!
San Francisco’s Non-Existent Contact Tracing
 To put it bluntly, Mayor Breed and Director of Public Health Grant Colfax appear to be deliberately misleading San Franciscans about the City’s efforts involving contact tracing of people who acquired COVID-19. To repeat, on March 27 Breed submitted a letter to the U.S. Department of Health and Human Services, and sent courtesy copies of her letter to Vice President Mike Pence, Speaker of the House Nancy Pelosi, U.S. Senators Feinstein and Kamala Harris, Congresswoman Jackie Spier, and Governor Gavin Newsom, specifically requesting support for the COVID-19 outbreak at Laguna Honda Hospital. Perhaps Breed thought that name dropping the names of five prominent Democrats might get the Republican-controlled U.S. DHHS to respond.
To put it bluntly, Mayor Breed and Director of Public Health Grant Colfax appear to be deliberately misleading San Franciscans about the City’s efforts involving contact tracing of people who acquired COVID-19. To repeat, on March 27 Breed submitted a letter to the U.S. Department of Health and Human Services, and sent courtesy copies of her letter to Vice President Mike Pence, Speaker of the House Nancy Pelosi, U.S. Senators Feinstein and Kamala Harris, Congresswoman Jackie Spier, and Governor Gavin Newsom, specifically requesting support for the COVID-19 outbreak at Laguna Honda Hospital. Perhaps Breed thought that name dropping the names of five prominent Democrats might get the Republican-controlled U.S. DHHS to respond.
At that point, one resident and six staff had tested COVID-19 positive at LHH.
 Breed brazenly requested on March 27 that the fed’s send 110 federal staff — including four infection control registered nurses; 10 additional professionals to conduct contact tracing; five respiratory therapists; 20 other healthcare testing workers; four epidemiologists; two laboratory staff; and five medical doctors, 30 RN’s, 10 LVN’s, and 20 personal care aides — all “to slow the spread of COVID-19 [and protect] our vulnerable skilled nursing residents and healthcare workers.”
Breed brazenly requested on March 27 that the fed’s send 110 federal staff — including four infection control registered nurses; 10 additional professionals to conduct contact tracing; five respiratory therapists; 20 other healthcare testing workers; four epidemiologists; two laboratory staff; and five medical doctors, 30 RN’s, 10 LVN’s, and 20 personal care aides — all “to slow the spread of COVID-19 [and protect] our vulnerable skilled nursing residents and healthcare workers.”
It’s a wonder Breed didn’t ask that the kitchen sink, a partridge in a pear tree, two turtle doves, three French hens, eight maids a milking, and ten lords a leaping also be thrown in for good measure, as long as she was begging for external help.
When did the federal government have enough on-hand staffing to divert 110 federal workers to a single jurisdiction? What about the additional 16 jurisdictions around the country that have populations nearly the size of San Francisco or larger, who may also have needed external staffing support help from the feds? Clearly, the feds didn’t have 1,760 extra staff on hand to send 110 staff to each of those 16 jurisdictions. What was Breed thinking? Or was this an exercise in sheer gluttony?
Four days after Breed submitted her letter, KCBS Radio reported on March 31 that Breed announced she had received just six doctors from the state and feds — not 110 additional staff. Then she bemoaned the six were “not nearly enough to get us to a better place in regard to Laguna Honda Hospital.” Ironically, Breed was lucky to get even six doctors; the feds could have sent her six geese a laying, instead.
Sadly, Dr. Colfax claimed on April 15 — two weeks after Breed failed to procure additional contact tracing resources from the state and federal governments — that San Francisco was belatedly ramping up contact tracing. Colfax offered no explanation about how the contact tracing personnel had been acquired, other than announcing the City is now belatedly training City employees such as librarians as disaster service workers to do the contact tracing normally provided by Department of Public Health employees. We have seen little data on how the contact tracing is progressing.
Colfax’s April 15 claim occurred the same day that the San Francisco Examiner reported Dr. Tomás Aragón — the official Health Officer for the City and County of San Francisco — lamented in March that a lack of investment in public health has limited San Francisco’s ability to conduct contact tracing investigations. The Examiner reported that Aragón had said:
“We don’t have enough [staff] to do syphilis contact [tracking] investigation. “We are down to the bare bones of public health infrastructure.”
—Tomás Aragón, MD, DrPH, County Health Officer
May 20, 2020
First, nobody believes the Department of Public Health is down to bare bones anything, except perhaps for DPH’s just six bare bones Respiratory Care Practitioners in job classification code 2536 (during a respiratory pandemic known as COVID-19) on the City payroll ending June 30, 2019 who were paid a mere $277,855 in combined salaries, and accounted for just 3.3 full-time equivalent employees based on their total number of hours worked.
By contrast, DPH’s payroll ending in June 2019 included 18 fat-cat Clinical Nurse Specialists (CNS) in job classification code 2323 — including LHH’s disgraced CEO, Mivic Hirose, who was removed from her job as a result of the patient abuse scandal at LHH last June but remains on the City payroll — at a cost of $3.9 million in base salaries. The 18 Nurse Specialists accounted for 17.9 FTE’s based on their total number of hours worked. We have nearly six times as many FTE’s doing Clinical Nurse Specialist work than we have Respiratory Care therapists.
You can almost bet that DPH’s 18 Clinical Nurse Specialists are not providing either respiratory care, or any direct patient care at all! I know from my decade working at Laguna Honda Hospital that the CNS’ do not provide direct patient care; they sit in offices and create various “make work” nursing programs.
 I have an idea: Since the 18 Clinical Nurse Specialists are largely doing desk jobs pushing paperwork for DPH, why not re-assign them to being part of DPH’s contact tracing workforce — you know, as disaster service workers ? That way, Breed wouldn’t have to burden the feds for staffing that she and former Mayor’s should never have trimmed back to bare bones status over the years.
I have an idea: Since the 18 Clinical Nurse Specialists are largely doing desk jobs pushing paperwork for DPH, why not re-assign them to being part of DPH’s contact tracing workforce — you know, as disaster service workers ? That way, Breed wouldn’t have to burden the feds for staffing that she and former Mayor’s should never have trimmed back to bare bones status over the years.
Second, if we don’t have enough resources to do contact tracing for syphilis, how the hell do Colfax and Breed now expect anyone to believe San Francisco is suddenly ramped up to do adequate COVID-19 contact tracing? Particularly in the absence of not having re-assigned those 18 Clinical Nurse Specialists to staff the ramparts.
I have an admission to make, ’lo 40 years later. Back in 1971 or 1972, when I was sowing my oats coming out of the closet as a young man, I was startled (and later ashamed) when I first received a phone call, followed by an in-person visit to my apartment, from Milwaukee’s Department of Public Health, informing me that through contact tracing it had received a report that I may have been infected with syphilis (or worse, I had infected someone else with it). I was of course mortified that the government — Big Brother — could track me down over a sexually-transmitted disease. It took me awhile before I was grateful that they had! And for the compassion they had shown me. If Milwaukee could do so in 1972, why can’t San Francisco now?
 To the extent that Newsom’s and Breed’s plans to loosen their social- and public-distancing and their shelter-in-place orders hinge on increasing contact tracing and greatly expanded testing, we’re off to a very rocky start!
To the extent that Newsom’s and Breed’s plans to loosen their social- and public-distancing and their shelter-in-place orders hinge on increasing contact tracing and greatly expanded testing, we’re off to a very rocky start!
Two months after Breed received the six federal doctors on March 31, the number of COVID infections at LHH soared ten-fold by June 7 to 71 cases — 46 staff and 25 residents. Apparently, the six federal staff — with or without the assistance from a partridge in a pear tree, two turtle doves, or eight maids a milking — and the expanded contact tracing proved to be ineffective at slowing the ten-fold COVID-19 tsunami that swept through Laguna Honda Hospital.
False Negatives, and Retesting
 All along, there have been concerns the true number of COVID-19 infections may be unknown, in part due to the problem of false-negative test results. Since mid-April, even China admits that preliminary research suggests the most common form of COVID-19 test produces false negative results 15% to 30% of the time. Most PCR tests undergo years of lab testing before they are used. With COVID-19, there wasn’t that kind of time before the COVID-19 tests were pressed into use.
All along, there have been concerns the true number of COVID-19 infections may be unknown, in part due to the problem of false-negative test results. Since mid-April, even China admits that preliminary research suggests the most common form of COVID-19 test produces false negative results 15% to 30% of the time. Most PCR tests undergo years of lab testing before they are used. With COVID-19, there wasn’t that kind of time before the COVID-19 tests were pressed into use.
If someone tests negative for COVID-19, it only means they probably weren’t infected at the time their specimen was collected. They may have been very early in their stages of infection at the time their specimen was collected.
Preliminary research indicates that common tests for COVID-19 may produce false negative results up to 30 percent of the time, and the inaccuracies are probably caused by the collection of samples, not the actual laboratory testing. In part, that’s because sample collection relies on using swabs placed in the back of the nose and mouth where it may be difficult to get to the place where the virus is located and hiding out, and collect a reliable sample.
Some experts in laboratory medicine express concerns the false-negative rate could be even higher.
On May 15, ABC’s World News Tonight with David Muir reported that a new analysis conducted by Johns Hopkins University shows there is a small window in which to obtain accurate test results. It is not only important to get tested; it also may be important when you get tested. The analysis noted that:
It’s not yet clear if the John Hopkins study applies only to the rapid, 15-minute point-of-care COVID-19 test produced by Abbott Laboratories — ID NOW — initially used by the White House, or if all PCR-based tests have the same narrow window of test accuracy.
False negatives can occur using different PCR tests, meaning they’re more useful for confirming the presence of an infection rather than giving a patient the all-clear. People who test negative are advised to have a retest.
False negative tests can occur if a specimen is not properly obtained, or if a patient was tested too early or too late in their infection. Laboratory error is also a possible cause of false negative test results. The PCR tests currently being used to diagnose active cases of COVID-19 can only indicate the presence of the virus material during the period of active infection. The tests do not indicate if a person was infected and subsequently recovered.
 The Johns Hopkins analysis also found that Abbott’s test missed one-third of infections when sample swabs were stored in chemicals meant to preserve samples, and more than 48 percent when sample swabs were kept dry.
The Johns Hopkins analysis also found that Abbott’s test missed one-third of infections when sample swabs were stored in chemicals meant to preserve samples, and more than 48 percent when sample swabs were kept dry.
On Thursday, May 14, the FDA posted a public alert on its web site stating that Abbott’s test might return false-negative results that “may need to be confirmed” by other testing methods, including a high-sensitivity authorized molecular test.
On May 8, news surfaced that Pence’s press secretary Katie Miller (wife of Stephen Miller, Trump’s speechwriter) had tested positive for COVID-19. Trump noted that Ms. Miller had tested negative “for a very long period of time,” including testing negative on Thursday, May 7 before she suddenly tested positive on Friday, May 8. There were no reports of how many times she had tested negative, or whether she had been tested with the Abbott ID NOW test.
 Strangely, the White House, Pence, and Trump have all been completely silent on whether all of Ms. Miller’s previous negative test results were actually false negatives, and whether she may have actually been positive and asymptomatic for several days while she wandered around the White House. For that matter, it may not have dawned on anyone in the White House to wonder how many other White House staff may have also repeatedly received false negative test results.
Strangely, the White House, Pence, and Trump have all been completely silent on whether all of Ms. Miller’s previous negative test results were actually false negatives, and whether she may have actually been positive and asymptomatic for several days while she wandered around the White House. For that matter, it may not have dawned on anyone in the White House to wonder how many other White House staff may have also repeatedly received false negative test results.
It isn’t known whether either Mayor Breed or Governor Newsom are factoring in the probability of a significant number of false negative test results in their race to re-open the City and the state. Those false negative test results may be contributing to the failure of flattening the curves.
Nursing Homes Seek Legal Immunity From Governor Newsom: A Cover-Up
As early as April 23, The Mercury News (formerly known as the San Jose Mercury News) published a scathing editorial calling on Governor Newsom to end the cover-up of COVID-19 nursing home deaths in California. Newsom had promised on April 10 to make addressing the threat of COVID in nursing homes his top priority. The Merc noted the most-basic tool for fighting any endemic or pandemic is accurate information, and without accurate information families have no way of knowing which facilities are safe, or unsafe. Obviously, a time of crisis is no time for information cutbacks.
 California’s reported nursing home data is believed to be grossly underestimated, given the paucity of data being released.
California’s reported nursing home data is believed to be grossly underestimated, given the paucity of data being released.
Part of the problem is that California’s Department of Public Health (CDPH) has chosen to hide running totals of patient and staff infections in each nursing home using a tool known as “de-identification,” in which facilities with less than 11 patients or 11 staff infections are reported simply as “<11,” escaping having to report actual aggregate facility-level data. CDPH claims the de-identification and the resulting data secrecy is to comply with the Health Insurance Portability and Accountability Act (HIPAA), the federal health privacy law to protect individual patient’s data. The HIPAA claim is just a pretext to avoid disclosing crucial data. There’s nothing in HIPAA that prohibits releasing aggregate data that doesn’t include patient identifiers. And it’s neither realistic nor plausible to believe that members of the public could glean the identity of any given patient from release of thousands of records rolled into a single raw number for a given facility.
But that’s a bogus claim Newsom is allowing to continue, because neither patient names nor their personal identifying information is released. So, the facilities, counties, and CDPH are essentially colluding in a cover-up, preventing Californians from learning which facilities have COVID outbreaks, how many cases they’ve had, how many deaths there have been in each facility, and whether the cases were among staff or residents. The Mercury News asserted this is fundamental public records information that should be updated and disclosed daily under the California Public Records Act (CPRA).
Here we are on June 8 — 81 days after Newsom issued his statewide shelter-in-place order on March 19 and 59 days since he promised on April 10 to make addressing the threat of COVID in nursing homes his top priority. All this time has slipped away, and we still don’t have an adequate sense of how widespread the COVID pandemic has hit California’s nursing homes and assisted living facilities at the facility level, and how hard they have been hit.
 On April 9, six organizations wrote to Governor Newsom requesting that he issue an executive order granting blanket immunity for health care providers and facilities. They also asked that all current state statutes and regulations be waived to achieve blanket immunity for them.
On April 9, six organizations wrote to Governor Newsom requesting that he issue an executive order granting blanket immunity for health care providers and facilities. They also asked that all current state statutes and regulations be waived to achieve blanket immunity for them.
The six organizations were seeking an overly-broad get-out-of-jail-free card from all administrative, criminal, and civil liability for any injury or death as a result of the COVID-19 pandemic. But they went further, requesting immunity for non-COVID problems, too.
The proposed overly-broad executive order would cover both reckless elder and dependent abuse situations as well as non- COVID-related negligence in any health care setting, without adequate public oversight of how many deaths in nursing homes were caused by criminal negligence. The industry-authored immunity proposal would permit anything a provider does or neglects to do, including mistreatment of non-COVID patients, to have no legal consequences.
It’s clear that the executive order being sought is designed to protect the nursing home industry and its profits, not to protect the lives of elderly patients.
The six agencies included three trade associations for physicians, hospitals, and health insurance plans (including the California Medical Association representing physicians; the California Association of Health Plans representing insurance plans; and the California Hospital Association, representing about 400 hospitals and is an organization closely affiliated with the Hospital Council of Northern and Central California). The three organizations have a vested interest in helping hospitals resume performing elective procedures — rather than in providing COVID care — in order to increase profit margins in hospitals.
The three additional organizations who petitioned Newsom included the California Assisted Living Association, representing various assisted living and continuing care retirement communities; Leading Age California, which represents assisted living facilities, affordable housing providers, and skilled nursing and community-based care facilities; and the California Association of Health Facilities, another trade association representing skilled nursing and intermediate care facilities for people with developmental disabilities.
Their April 9 letter was shocking, in part, because San Francisco’s Department of Public Health had just rolled out it’s preliminary on-line “COVID-19 Tracker” web site just two days earlier, on April 7, which initially reported 622 COVID cases citywide and nine COVID-related deaths.
The six agencies must have known public accountability and public records transparency were coming their way, and wanted Newsom to step in to shore up liability protections. It should be noted that the April 9 letter to the Governor came just 21 days after Newsom had issued his statewide shelter-in-place order on March 19, but before members of the public began to learn on April 17 just how widespread the COVID-19 pandemic had become in California.
 In retrospect, the April 9 letter seeking broad immunity was also shocking because it was sent to Newsom eight calendar days before the California Department of Public Health (CDPH) launched its own COVID-19 web site on April 17 beginning to report the number of COVID infections among nursing home staff and residents, which then stood at 3,000 infections. CDPH would take longer before it started the number of deaths of nursing home staff and residents.
In retrospect, the April 9 letter seeking broad immunity was also shocking because it was sent to Newsom eight calendar days before the California Department of Public Health (CDPH) launched its own COVID-19 web site on April 17 beginning to report the number of COVID infections among nursing home staff and residents, which then stood at 3,000 infections. CDPH would take longer before it started the number of deaths of nursing home staff and residents.
By April 9, California had 19,691 COVID cases and 538 COVID-related reported deaths, even before we were told how many of the cases were in skilled nursing and assisted living facilities. By the time the public learned of CDPH’s new web site reporting facility-level COVID data on April 17, the number of COVID cases statewide rose to 29,154 cases and 1,037 COVID-related reported deaths — in just the eight days after the six agencies begged Newsom for absolute legal immunity.
 It’s a fair assumption that the six trade associations and their lobbyists seeking immunity from Newsom knew from their own quality management staff, risk management staff, or their member hospitals’ infection control and utilization management staff that they all had a tsunami-level problem on their hands, long before — perhaps for weeks — their April 9 letter to Newsom.
It’s a fair assumption that the six trade associations and their lobbyists seeking immunity from Newsom knew from their own quality management staff, risk management staff, or their member hospitals’ infection control and utilization management staff that they all had a tsunami-level problem on their hands, long before — perhaps for weeks — their April 9 letter to Newsom.
By April 28, when data reporting became somewhat more accurate, of the 1,862 statewide COVID-related deaths 792 (42.5%) occurred in skilled nursing and RCFE facilities across the state.
Luckily, 17 organizations submitted a letter to Governor Newsom on April 23 opposing the immunity request. The 17 organizations included Justice in Aging, ACLU-California, California Advocates for Nursing Home Reform (CANHR), Disability Rights California, Disability Rights Education and Defense Fund, National Health Law Program, the Western Center of Law and Poverty, and ten additional organizations.
They noted there is no legitimate public policy reason to grant such broad immunity:
“The extent of the requested immunity is staggering: Complete immunity for all negligence, whether or not related to a shortage of equipment and, in fact, whether or not related to COVID-19. There is no legitimate public policy reason to completely release health care providers from responsibility for their own negligent or reckless actions or behavior.”
The letter also noted that granting immunity is unnecessary even for health care impacted by COVID-19, because existing laws regarding negligence already require that circumstances be considered to determine liability.
The 17 organizations respectfully requested that Newsom not grant immunity for health care providers, since existing legal standards already in place are designed to account for any “surrounding” circumstances. Granting them immunity would send a signal of improperly valuing providers more than the lives of their patients.
To date, Newsom has not issued any such immunity order, but patient advocates remain fearful that he will. Nursing homes should not be shielded from accountability via blanket immunity!
COVID First Wave Isn't Over
Breed was right, of course, when she noted on May 6 that San Francisco had not flattened its COVID curve. We’re still not through the first wave. But Breed continues to prematurely re-open various types of businesses in San Francisco.
Newsom, for his part, is painfully aware that California’s first wave isn’t over, either. He said so during his weekly COVID press conference on June 22. But he’s sending mixed messages, since on June 10 Newsom claimed there is no turning back on plans to re-open the State.
Of note, between June 10 and June 22, there were an additional 648 COVID-related deaths, pushing California’s COVID death toll to 5,523. And between June 10 and June 22, an additional 38,926 COVID cases were diagnosed, fully 21.7% of California’s now 179,605 total COVID cases. Those increases over that 12-day period should be telling Newsom he should turn back his plans to re-open the State.
 Newsom did indicate on June 22 that if there’s a surge in COVID cases, the State could dial back and re-impose the shelter-in-place orders.
Newsom did indicate on June 22 that if there’s a surge in COVID cases, the State could dial back and re-impose the shelter-in-place orders.
Breed and Newsom appear to be far too impatient and may be re-opening the City and the State far too soon.
As of June 23, there have been at least 23,530 patient and staff COVID-19 infections in California SNF’s and RCFE’s. There have been 91 deaths of SNF staff, 2,348 deaths of SNF patients, and 406 deaths of staff and residents in California RCFE’s, totaling a minimum of 2,845 premature COVID-19 deaths in various types of elder care facilities — 51% of California’s 5,577 COVID-related deaths through June 23.
 Each of those 5,577 people had names, families, and life stories, and they, too, may have wanted to achieve immortality through not dying, like Woody Allen and Berenice.
Each of those 5,577 people had names, families, and life stories, and they, too, may have wanted to achieve immortality through not dying, like Woody Allen and Berenice.
In San Francisco and elsewhere around the world, COVID-19’s impact on people of color has been dramatic: As of June 22, of San Francisco’s now 3,185 COVID cases, 50.1% were among Hispanic residents, who make up roughly 15% of San Francisco’s population. Of the 3,185 COVID cases in San Francisco, 11.9% were among Asian-Americans, but of the now 48 deaths in the City through June 22, 45.8% (22) of the deaths were Asian-Americans.
Sadly, these alarming numbers only include the first wave of COVID, even before we get to a second wave next fall.
Trump has been hawking nonsense since May that without testing there wouldn’t be so many known cases, when he claimed “It could be that testing is over-rated. If we didn’t do any testing, we would have very few [COVID] cases” As Rachel Maddow noted in May, without the testing Trump would have had the same number of COVID cases (if not more), but he — and the rest of the nation — just wouldn’t know about them, as if ignorance is bliss.
 A month later, Trump returned to beating the same dead horse. “If we stop testing right now, we’d have very few cases, if any,” Trump said on June 15 during an event for seniors at the White House.
A month later, Trump returned to beating the same dead horse. “If we stop testing right now, we’d have very few cases, if any,” Trump said on June 15 during an event for seniors at the White House.
Trump even pushed Vice Poodle Pence into encouraging state governors during a June 15 conference call to adopt the administration’s claim that increased testing helps account for the new coronavirus outbreak reports, even though evidence has shown that the explanation is deliberately misleading.
At his re-election kick-off rally (Part 2) in Tulsa, Trump returned to trying to push the same water uphill, saying:
“Testing is a double-edged sword. When you do testing to that extent, you’re going to find more people; you’re going to find more cases. So, I said to my people, ‘Slow the testing down, please’.”
— Donald J. Trump
June 20, 2020
The White House tried to walk Trump’s nonsense back, pathetically claiming he was “just kidding.” But on June 23, Trump clearly stated “I don’t kid [around].” News surfaced Wednesday, June 24 that the Trump administration is set to end federal funding for 13 COVID-19 testing sites on June 30 in five states: Illinois, New Jersey, Colorado, Pennsylvania, and Texas. Indeed, he’s not kidding and if he gets away with ending that federal funding it won’t be long before he tries to end all federal funding for COVID testing, and not just in those five states.
Obviously (unless you’re Trump) federally-funded and federally-supported testing sites remain critically needed, particularly as new COVID-19 hotspots are identified.
It’s as if Trump, Pence, and their voter “base” really believe that either 1) The coronavirus is smart enough to only infect, sicken, and kill people who received a COVID-19 test, and their resulting illnesses and deaths were brought on because the virus was smart enough to know the victims had been stupid enough to seek getting a test; 2) The virus is smart enough to skip biting you if you haven’t received a test; or 3) That stopping testing would simply result in fewer COVID cases, COVID would magically go away completely, or COVID would hop an international flight back to Wuhan (most likely another misguided Trump conspiracy theory).
 Clearly, most graduates of Wharton Business School (except perhaps Trump) understand that any effort to restrict testing will mean more Americans will lose their lives. That suggests that deliberately withholding testing that could end up saving lives borders on criminal behavior, at least in my book. Maybe Trump was the dumbest person to graduate from Wharton.
Clearly, most graduates of Wharton Business School (except perhaps Trump) understand that any effort to restrict testing will mean more Americans will lose their lives. That suggests that deliberately withholding testing that could end up saving lives borders on criminal behavior, at least in my book. Maybe Trump was the dumbest person to graduate from Wharton.
Sunshine, Sunlight: The Best Disinfectant
On June 12, Rachel Maddow interviewed David Grabowski, MD, a healthcare policy professor at Harvard Medical School. News had surfaced during a hearing indicating there had been at least 40,000 COVID-related deaths in nursing homes nation- wide, but Grabowski believes that number is a wild underestimate and we still don’t have a full count of the actual number of nursing home COVID deaths, in part because data collection at the start of the pandemic was a huge problem.
 Maddow and Grabowski believe the federal government was derelict in its nursing home corona virus response.
Maddow and Grabowski believe the federal government was derelict in its nursing home corona virus response.
Figure 5: Nursing Home Deaths Increase
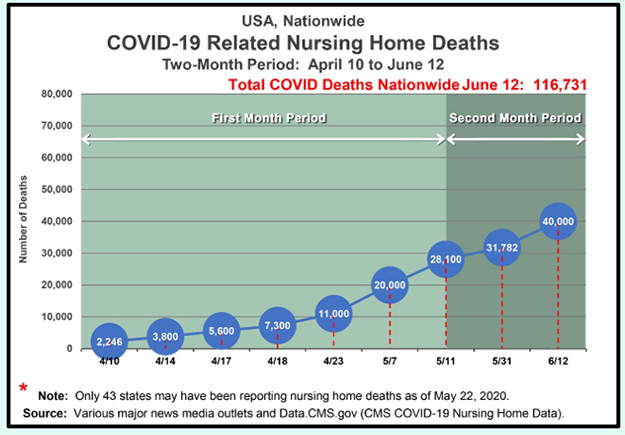
Grabowski said the federal government should have been delivering usable personal protective equipment (PPE) to nursing homes but failed to do so, even though PPE is the number one weapon to fight COVID in nursing homes and robust testing is the number two weapon.
Grabowski believes we are in the same position with nursing homes that we were in four months ago, in March, when our national nightmare began! Clearly, nursing facility residents and staff deserve better.
If we want to contain coronavirus in this country, it has to start in nursing homes, since that’s where the greatest number of deaths are.
Secrecy and misinformation from the highest levels of government have worsened the affects from COVID-19. But failure to take a hard look at our response as a nation is naive and dangerous, and will leave us vulnerable to similar or worse outcomes during future pandemics.
 Although sunlight may not be the best disinfectant, when it comes to the coronavirus by shining a light on our response, and guaranteeing transparency around future preparedness, we can begin to treat the disease of indifference that has infected our democratic institutions.
Although sunlight may not be the best disinfectant, when it comes to the coronavirus by shining a light on our response, and guaranteeing transparency around future preparedness, we can begin to treat the disease of indifference that has infected our democratic institutions.
Forbes was right: The most important statistic is that well over 42% of COVID-related deaths in the U.S. have come from the 0.6% of the nation’s population living in nursing homes. None of these lives were “disposable” or “expendable.”
Since COVID-19 is a deadly respiratory illness affecting people’s ability to breathe, I’m haunted wondering how many of the 2,845 people who have died in California nursing facilities through June 23 uttered “I can’t breathe” as their last words.
Like Dr. Palmer, I want answers, too!
Full Disclosure: My decade of employment at Laguna Honda Hospital overlapped Dr. Palmer’s stellar career there.
Monette-Shaw is a columnist for San Francisco’s Westside Observer newspaper, and a member of the California First Amendment Coalition (FAC) and the ACLU. He operates stopLHHdownsize.com. Contact him at monette-shaw@westsideobserver.com.
1 To access COVID-19 data involving RCFE and ARF facilities on the California DSS web site, scroll down to the link “NEW: COVID-19 Positive Cases in Adult and Senior Care Facilities.”