 September 12, 2022
September 12, 2022Taking Ownership of SFDPH's Mistakes
Rising Costs to Rescue Laguna Honda Hospital
September 12, 2022
Taking Ownership of SFDPH's Mistakes
Rising Costs to Rescue Laguna Honda Hospital
Potential Bombshell News:
LHH Was Following State Acute Care Hospital Regulations, Not
Federal Long-Term Care Skilled Nursing Facility Regulations
Failure to Implement “Critical Element Pathways” Education
May Have Affected LHH’s Loss of CMS Certification
by Patrick Monette-Shaw
All advocates and San Franciscans who support Laguna Honda Hospital and Rehabilitation Center (LHH) want — above all else —our beloved skilled nursing facility to remain open.
They want to secure re-certification of LHH by the Centers for Medicare and Medicaid (CMS) to resume receiving federal funding to rescue the hospital and preserve its mission to care for the most vulnerable among us, particularly elderly and disabled residents who rely on Medi-Cal funding for healthcare in their time of great need.
We all knew this might come with a hefty price tag. But just how large will that price tag grow?
How could LHH have not implemented training on CMS’ “Critical Element Pathways” program before now, and how could LHH have been following the wrong Federal and State regulatory guidelines?
Escalating Consultant Costs
As Dr. Derek Kerr first reported in the Westside Observer on June 22, 2022, the San Francisco Department of Public Health (SFDPH) — through its governing body, the Health Commission — approved two contracts with external consultants hired to guide LHH back through the process of re-gaining CMS certification. One contract with Health Management Associates was for $3.7 million, and a second contract with Health Services Advisory Group (HSAG) was for $1.8 million, for a combined cost of $5.5 million.
Two months later, the Health Commission’s August 2 agenda announced a third contract with Tryfacta, Inc. to provide as-needed staffing during the LHH Re-certification Project for the period June 17, 2022 to December 31, 2023, which I reported for the Westside Observer on August 17, 2022. [It turns out the December 31, 2023 ending date for the Tryfacta contract listed on the Health Commission’s meeting agenda was an error by the Health Commission’s Secretary; the initial Tryfacta contract is set to run only until December 17, 2022.]
The as-needed staffing contract with Tryfacta has an immediate need to hire seven full-time equivalent (FTE) dieticians and two Dietetic Technician’s FTE’s. The contract specifies there may be optional or future needs to hire 14 other types of clinical occupations, including Registered Nurses, Certified Nursing Assistants and Certified Medical Assistants, Pharmacists, Social Workers, and Physicians, among others, but didn’t indicate how many FTE’s in each job classification category may be needed.
More news about the LHH contracts broke on September 1 when the Board of Supervisors meeting agenda for Tuesday, September 6 was posted on-line. It turns out all three of the contracts to assist LHH had not yet been approved by the Board of Supervisors, and were introduced for retroactive approval on September 6. The Board did not vote on the three contracts on September 6, because they still face a hearing before the Board’s Budget and Finance Committee for potential approval.
But disturbingly, the initial HSAG contract is already seeing its first amendment, increasing the contract by $5.2 million to a total of $6,989,564 — just $10,000 shy of $7 million.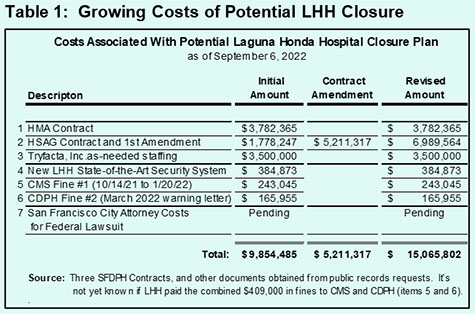
That brings the three consulting contracts to a total of $14.4 million. There are $793,873 in other known costs of the LHH crisis, shown in Table 1, pushing total costs of the LHH crisis to date to $15 million, and counting. That $15 million represents a 172.7 percent change increase within just over two months from the $5.5 million in costs for the first two consulting contracts we learned about from Dr. Kerr in June.
Those costs could get much worse, because the Board of Supervisors was presented on September 6 with the three Resolutions that were introduced by the Department of Public Health on August 12, 2022 while the full Board was out for its August recess. All three Resolutions were referred to the Board’s Budget and Finance Committee but have not yet been scheduled for Committee-level public hearings.
The three Resolutions involve retroactive approval of the HMA contract, the HSAG contract and its first contract Amendment, and the Tryfacta contract.
Of interest, the $5.2 million HSAG contract amendment includes $ 1,468,800 (28.25 percent of the $5.2 million total) for two of LHH’s new positions — an apparently licensed Nursing Home Administrator (NHA) and a licensed Assistant Nursing Home Administrator (AHNA). HSAG’s contract amendment itemizes 3,672 hours being billed at $400 an hour for the two positions, but it’s not clear or known yet whether that is to “rent” HSAG consultant staff to fill those two positions on an interim basis, or whether the contract is for training costs to educate LHH new employees who may have already been hired to fill those two positions. On the one hand, it sounds like LHH may take until the end of 2022 to recruit and hire employees for the two positions. On the other hand, SFDPH and LHH staff have not been forthcoming answering public records requests about the question of whether LHH has actually hired the HMA and AHNA positions, or whether LHH is just “renting” HSAG through December 17 to fill the two positions temporarily.
Nor has SFDPH indicated whether there will be additional HSAG contract amendments to continue providing HSAG consultant staffing to fill the NHA and ANHA positions, or training LHH staff following December 17, 2022, when HSAG’s contract is set to end — assuming LHH may not hire staff to fill those two positions by December.
Trojan Horse Caveat in the Three Resolutions
Unfortunately, each of the contracts with the three consultants contained a potential Trojan Horse dancing through the legislative language, similar to the following:
“ … and to authorize the Department of Public Health to enter into any amendments or modifications to the contract that do not otherwise materially increase the obligations or liabilities to the City and are necessary or advisable to effectuate the purposes of the contract or this Resolution. …
FURTHER RESOLVED, That the Board of Supervisors authorizes DPH to extend the term and/or increase the amount of the agreement, not to exceed ten (10) years or $10,000,000, to the extent that DPH determines, in consultation with the City Attorney, that such modification is in the best interests of the City, does not otherwise materially increase the obligations or liabilities of the City, is necessary or advisable to effectuate the purposes of the agreement, and is in compliance with all applicable laws; … ”
Although the language said SFDPH couldn’t materially increase the “obligations” of each contract, the language also seemed to authorize SFDPH that it could raise each contract to not exceed $10 million.
One knowledgeable observer believed this may have provided wiggle room for SFDPH to increase each of the three contracts to $9,999,999 — a dollar shy of each $10 million-per-contract threshold — that might push the contracts to $29,999,997, without SFDPH having to come back to the Board of Supervisors for approval to increase the costs of the three contracts.
The possibility that the current $14.2 million total costs of the three contracts might be raised to a total of $30 million seemed excessive to most observers, even to all of us who want LHH to be saved and preserved for future generations.
The Westside Observer alerted City Hall that the three contracts could be increased to $10 million each. Sources indicated on September 7 that the legislative language allowing these excessive increases will be removed from the proposed Resolutions when they are heard by the Board of Supervisors’ Budget and Finance Committee. We’ll see if that actually occurs. The three Resolutions were not scheduled for the Budget Committee’s weekly meeting on September 14. It will take ongoing vigilance by community advocates to monitor whether SFDPH will come back again and propose increasing the contract amounts through additional contract amendments at a later date.
LHH’s History of Incompetent Management
The current crisis facing LHH that began in October 2021 and resulted in LHH losing it CMS certification and loss of federal reimbursement in April follows a long history of incompetent management at Laguna Honda Hospital. For instance, back in 2019 a scandal involving patient sexual abuse at LHH that dated back to 2016 erupted, forcing the ouster of LHH’s then-Chief Executive Officer, Mivic Hirose.
As I reported for the Westside Observer in December 2019, when Hirose was fingered along with other LHH “leaders” as having contributed to the lax environment that contributed to the patient sexual abuse at LHH, she reportedly bemoaned the fact that under her own leadership, LHH did not have a “culture of patient safety,” when in fact LHH celebrates the national Patient Safety Awareness Week annually. It had been Hirose’s job to instill that culture of safety among her own nursing staff.
After all patient safety is precisely why CMS and State inspection surveyors routinely inspect nursing homes in the first place.
Instead, Hirose instilled a culture of silence, which remains an on-going problem at LHH to this day. As I noted in 2019, “A culture of patient safety is particularly vulnerable to fatality if it collides with a culture of silence speeding out of control, careening throughout a hospital for over a decade-and-a-half.”
LHH’s patient sexual abuse scandal in 2019 has cost the City $1.8 million between fines and lawsuit settlements. But that amount will likely rise, because only one of the three patients who filed lawsuits involving their sexual abuse at LHH has been settled, for $800,000. The other two lawsuits have not yet been settled, or announced by the City.
LHH’s lack of a culture of patient safety is still ongoing, as witnessed by the recent events we have been reporting on in the Westside Observer since May regarding the threat of closing LHH.
As my 2019 article noted, Hirose began her career at SFGH in 1985 as a Medical-Surgical Staff Nurse, and became SFGH’s Medical/Surgical Nursing Director in 1999. In 1999 Hirose transferred to LHH and became LHH’s co-Director of Nursing. She’s essentially a SFGH management transplant, like many other senior managers at LHH.
Take John Kanaley.
Way back in 2003 and 2004, then-Director of Public Health Mitch Katz instituted his disastrous “flow project” to discharge dangerous, robust behaviorally challenged younger patients from SFGH into LHH, mixing them in with elderly vulnerable patients, many of whom had dementia’s, creating a volatile milieu for both patient populations. Katz forced LHH’s Medical Director, Dr. Terry Hill, to resign, eliminated Mary Louise Fleming’s position as LHH’s Director of Nursing, and ousted LHH’s then Executive Administrator, Larry Funk.
Katz appointed John Kanaley as Funk’s replacement in November 2004. There were serious concerns about Kanaley’s appointment, given his lack of credentials and qualifications. Kanaley’s prior job experience was in facilities management, not hospital administration, and certainly not as a Nursing Home Administrator, as Funk had been. Like Hirose, Kanaley had no experience working in a skilled nursing facility environment. Katz reportedly told a contingent of senior LHH staff that it didn’t matter because he wanted somebody who would “kick the [LHH] doctor’s asses.”
Hirose was forced to resign as LHH’s CEO, but managed to land a cushy Golden Parachute job with San Francisco’s Department of Public Health. In the fiscal year that just ended on June 30, 2022 (FY 2021–2022), Hirose managed to earn $248,600 in total pay as a Clinical Nurse Specialist. [Clinical nurse specialists typically are not involved in direct patient care in any way.] LHH’s then-Quality Management Director (Regina Gomez) and then-Director of Nursing (Madonna Valencia) were also forced out, and replaced by SFGH staff, at least temporarily.
And when LHH’s replacement CEO, Michael Phillips, was forced out in June 2022 — with the apparent approval and consent of SFDPH’s current Director of Public Health, Grant Colfax — he too was replaced by another SFGH long-time employee, Roland Pickens, who has a 20-plus year career at SFGH, including as SFGH’s Chief Operating Officer.
This long history of SFGH management transplants came from a culture of running an acute-care hospital at SFGH, a totally different culture than running a long-term care skilled nursing facility. Unfortunately, the culture of acute-care management employees has exacerbated the culture of silence among nursing home trained staff too intimated by senior managers at LHH to speak out.
Much of LHH’s lack of culture of patient safety is related to the many ongoing state survey inspections involving what are known as “F-Tag” violations.
F-Tags and Critical Element Pathways
As I reported in the Westside Observer on July 19, LHH has known for years that if it violates CMS’ “Conditions of Participation” and receives substandard care F-tag violations, it could be decertified. As it was, LHH had passed its CMS and State inspection surveys for well over three decades.
I reported that when Congress passed the 1987 Omnibus Budget Reconciliation Act, CMS began developing rules and regulations for Skilled Nursing Facility (SNF) providers, to assure uniformity in survey processes of nursing facilities nationwide focused on guidance to protect the quality of care patients receive in SNF’s such as LHH, not arbitrary Kafkaesque rules. Those rules involved incremental development of 21 separate Federal Regulatory Group categories that apply to Long-Term Care (LTC) facilities regulated by CMS. Across all 21 regulatory groups applicable to LTC SNF’s, there are a total of 211 different named F-tags. [A recent “LTC F-Tags Phase 2 Crosswalk” file posted on CMS’ website suggests there may be up to 249 F-Tags.]
I reported F-Tags (a.k.a., Federal-tag number) correspond to a specific regulation included within a Code of Federal Regulations. For example, “F744” involves “Treatment/Service for Dementia” — a substandard quality of care deficiency — which refers to Federal Regulation 483.40 regarding “Behavioral Health.” The F-Tags help nursing home inspection surveyors categorize violations that impact nursing home residents.
LHH’s own staff and the Department of Public Health had to have known about the F-Tag rules for 35 years, that they had followed mostly uneventfully for well over two decades. After all, LHH has had a Department of Education and Training in its Nursing Department long before 1999 when I first started working there. The Nursing Department’s Education and Training staff should have been educating LHH employees about the various F-Tag requirements all these years in order to pass annual inspection surveys.
LHH’s Nursing Education and Training Department also should have known that CMS had rolled out and began implementing a new Critical Element Pathways (CEP) program in November 2017, when Mivic Hirose was still LHH’s CEO. Maybe Hirose was too busy implementing her culture of silence milieu among staff, and forgetting about developing a culture of patient safety to have noticed CMS’ new CEP program.
The CEP program appears to be under CMS’ Quality, Safety and Oversight Group in its Center for Clinical Standards and Quality. The Center for Clinical Standards and Quality/Quality, Safety and Oversight Group has been updating its “Revised Long-Term Care Surveyor Guidance” to State Survey Agency (SSA) Directors for nursing home survey inspectors — who in our case, are affiliated with the California Department of Public Health (CDPH) — given that the CEP’s have been being rolled out since 2017.
The CEP’s involve investigative protocols to inspect quality of patient care concerns that arise and are not otherwise uncovered when examining F-Tags violations. The CEP’s are used for investigating potential care areas of concern identified during on-site facility inspections. CMS is apparently still updating the CEP’s and expects to complete the updates for download from the CMS website by October 24, 2022.
The current 41 CEP’s include very detailed questions, and depending on the responses received the CEP’s then guide surveyors through potential F-Tag violations to cite, if appropriate. Two samples of the CEP’s include:
Bombshell News: LHH Had Been Utilizing Wrong Federal Guidelines
On August 16, LHH’s interim CEO, Roland Pickens made a PowerPoint presentation on the status of the “LHH Closure Plan and CMS Recertification” to the full Health Commission. In it, Pickens noted that LHH is undertaking three major education initiatives, including focusing on Critical Element Pathways (CEP), a relatively new program from CMS that state surveyors from California’s Department of Public Health (CDPH) use during on-site inspections of skilled nursing facilities in the State.
Pickens asserted the CEP program seeks to engage and support middle managers so they can support frontline staff. Pickens claimed Laguna Honda will continuously use CEP’s to reinforce staff education and assess current hospital practices against the CMS regulations and F-Tags.
One problem is that CMS’ CEP program is not “new.” It was developed long before CMS rolled it out in November 2017. Why LHH is just learning of the CEP processes five years after they were implemented and LHH is now implementing them in LHH’s educational arsenal wasn’t explained. And Pickens didn’t mention whether the CEP state surveyors may have apparently used since 2017 may have contributed to LHH having flunked its serial state inspections between November 2021 and April 14, 2022, setting off LHH’s current crisis. A Health Commissioner asked a pointed question to this effect, but Pickens dodged and deflected from answering the direct question on August 16.
During Pickens’ slide presentation, he first indicated (on videotape) that incorporating the CEP’s into LHH’s staff education curriculum will get LHH on the right track towards CMs recertification:
“[CEP’s are] basically a tool that high-functioning nursing facilities use to ensure that all staff at the skilled nursing facility are aware of what the requirements are, but also are aware of how they in their discipline or Departments are expected [to perform] to ensure that, overall, the skilled nursing facility maintains [CMS regulatory] compliance. So, these 39 critical pathways are being rolled out at Laguna. There are 39 and we’ll talk a little bit more about how we’re implementing those, roughly every week, we go through 10 of the 39, so that on a monthly basis, we’ve covered all 39 of those CEP’s every month at Laguna. It’s an on-going process and not a one-and-done. It’s baking into the fabric of Laguna Honda Hospital. This [is a] core element of using Critical Element Pathways, and these are the same tools that the [federal and state surveyors] use when they do the [inspection] surveys at Laguna. So, we feel confident by incorporating this as the pillar in staff education that we’re on the right track.”
Pickens was mistaken. There are not 39 CEP’s; there are 41 CEP’s.
Given the two examples of CEP’s in this article above — the Accidents CEP and the Rehabilitative or Restorative Services CEP — it is hard to believe that whichever LHH staff are being trained on the CEP’s can digest and fully comprehend their education about 10 different CEP’s each week. That may be an ambitious Johnny-come-lately, wishful-thinking goal in hoping to pass CMS’ rigorous recertification process.
Following Pickens’ slide show on August 16, Health Commissioner Tessie Guillermo specifically asked him whether the Critical Element Pathways may have played a role in previous regulatory inspection surveys of LHH. In effect, Guillermo was asking whether LHH’s failure to follow the CEP’s may have played a direct role in LHH flunking it inspection surveys, and whether that may have contributed to CMS decertifying LHH in April 2022. It’s a legitimate question … that deserves an honest answer.
Rather than answering Guillermo’s direct question, Pickens dodged answering, but blurted out a damning admission, however inadvertently, that LHH had been using the wrong regulatory guidelines:
“And an analogy would be that, you know, we’ve talked before that one of the findings that Laguna was structured more like an acute care hospital, so Laguna really focused on, for example, the State of California Title 22 [regulations]: For acute hospitals [are] driven by the Title 22 regulations and that’s okay if you’re a [general acute care hospital] — but Laguna is a skilled nursing facility. Like San Francisco General, they [LHH] utilize Title 22 general acute care hospital guidelines and the Joint Commission [on Accreditation of Hospital] guidelines as their pathways towards regulatory compliance. So, while Laguna wasn’t a Joint Commission survey [facility], but it [LHH has] a State of California license so it had been using Title 22 and not using the CEP [guidelines] which are the standards for skilled nursing facilities, and Laguna wasn’t using them. But now we are using the CEP’s [guidelines] and so, one would hope, one would think that perhaps had we been utilizing CEP’s in the past, perhaps, the facility could have been more in line with regulatory compliance and we’re moving forward to put that in place, because now we’ve learned and been educated that CEP’s are what high performing nursing homes use to maintain their [regulatory] compliance developed by CMS.”
There you have it: Pickens seems to have clearly acknowledged LHH had been following the wrong regulatory guidelines by using California’s Title 22 “Acute Care Hospital Guidelines,” not using CMS’ “Skilled Nursing Facility Regulatory Guidelines” and CMS’ CEP’s.
Pickens also clearly stated that “had we been utilizing CEP’s in the past, perhaps, the facility could have been more in line with regulatory compliance …”— say, between October 2021 and April 14, 2022 when LHH’s problems with state surveyors began and LHH lost it’s CMS certification — LHH might have come into compliance with CMS” regulatory guidelines, and might have prevented it being ordered to discharge and transfer all of LHH’s residents out of county.
The meeting minutes of the Commission’s August 16 meeting reported that Pickens also said “that prior to the current LHH consultants coming on board, CEPs were not on LHH’s radar. Instead, much of the LHH regulatory focus was on Title 22 acute hospital and Joint Commission guidelines. [Pickens] noted this was a deficit.”
For his part, Health Commissioner Edward Chow was quoted in the meeting minutes that “The LHH-JCC [the Health Commission’s LHH-Joint Conference Subcommittee] has been following the state regulatory results, but the existence of the CEPs was not mentioned in the JCC meetings until recently.”
This appears to be another damning admission that apparently even the Health Commission was unaware that CMS had rolled out and implemented the CEP program in November 2017, and that Pickens and senior members of LHH’s management team had not educated or mentioned to the three Health Commissioners assigned to the LHH-JCC “until recently” that LHH was going to rapidly focus on rolling out the CEP’s as part of LHH’s education arsenal to regain CMS certification!
That’s where the problem of LHH’s long culture of silence history comes in. To the extent LHH was following the wrong regulatory guidance of Title 22 acute-care hospital regulations, LHH’s Nursing Education and Training Department, LHH’s Director of Nursing (DON), LHH’s senior nursing department managers, and even LHH’s front-line nursing staff all should have spoken up and broken the culture of silence by saying something like: “Wait! We should be following CMS’ skilled nursing facility regulations, not Title 22.”
Apparently, the culture of silence is so ingrained and embedded at LHH that nobody spoke up … leading to LHH’s current dire situation.
The Board of Supervisors should investigate further and get a clear answer to Commissioner Guillermo’s direct question of whether the lack of implementing the Critical Element Pathways when CMS first rolled them out in 2017 may have played a role in previous regulatory inspection surveys of LHH, and whether that failure may have contributed to LHH losing its CMS certification.
After all, if the answer to that question is “Yes,” then anyone and everyone who was involved in not implementing the Critical Element Pathways program much earlier at LHH should also be terminated. It should not be just former LHH CEO Michael Phillips whose head rolled and was terminated. And if it involved Director of Public Health Grant Colfax, then he should be terminated, too.
As I wrote on the August 22 issue of the Westside Observer, former-District 1 Supervisor Sandra Lee Fewer had published a commentary in the August 5 Richmond Review/Sunset Beacon that SFDPH hadn’t taken ownership of the problems at LHH. Fewer had astutely noted that ““[The problems of substandard care at LHH] clearly could have been prevented and could have been remedied” and that “… [San Francisco’s] Department of Public Health and CMS need to own this …”
I agreed with Fewer that SFDPH hadn’t acknowledged ownership that it was itself responsible for the violations and potential closure of LHH, and it was long past time the health department and the Health Commission take ownership of its mistakes.
Perhaps Pickens’ admission to the Health Commission on August 16 — that the lack of implementing the Critical Element Pathways program at LHH earlier may have contributed to LHH’s decertification, and Pickens’ acknowledgement that LHH had been following the wrong regulatory guidelines by using California’s Title 22 “Acute Care Hospital Guidelines,” rather than using CMS’ “Skilled Nursing Facility Regulatory Guidelines” had been a major mistake — may have been the first step in LHH and SFDPH taking ownership of its past mistakes. We can only hope so.
Among other of LHH’s problems, its culture of silence must be stopped in order to end its substandard quality of patient care inspection violations!
Afterword
LHH’s CEO Roland Pickens is set to update the Health Commission’s LHH-JCC on Tuesday, September 13. Unfortunately, his PowerPoint presentation shows on pages 8 through 10 that as far as LHH’s CMS recertification preparation goes, three Weekly [CMS] “Survey Readiness and Compliance Assessments” show that as of September 2, LHH is not meeting 90% or
greater progress towards its goals:
This presentation about LHH’s preparedness for a CMS reinspection survey should alarm the three Health Commissioners assigned to the LHH-JCC, and should alarm both the full Health Commission and the City’s Board of Supervisors. After all, LHH’s problems in passing CMS and CDPH on-site survey inspections reared its ugly head in October 2021. We’re now just weeks shy of that one-year anniversary, and reportedly just weeks away from the CMS recertification survey inspections process to begin.
In addition, various vacancy reports for LHH’s staffing in the Executive Team report presented by Roland Pickens to the three Health Commissioners for the September 13, 2022 LHH-JCC (LHH Joint Conference Committee) meeting are alarming:
Given alarming staff vacancies and LHH’s high percentage of behaviorally challenged residents, how is LHH providing appropriate care for these residents safely?
Is this what San Franciscans are getting for its $15 million investment to date for the three consultant contracts designed to help guarantee LHH obtains CMS recertification?
Monette-Shaw is a columnist for San Francisco’s Westside Observer newspaper, and a retired City employee. He received a James Madison Freedom of Information Award in the “Advocacy” category from the Society of Professional Journalists–Northern California Chapter in 2012. He’s a member of the California First Amendment Coalition (FAC) and the ACLU. Contact him at monette-shaw@westsideobserver.com.