 October 13, 2022
October 13, 2022Ongoing Problems Threaten the Hospital’s Re-Certification
Worrisome Laguna Honda Hospital Issues
October 13, 2022
Ongoing Problems Threaten the Hospital’s Re-Certification
Worrisome Laguna Honda Hospital Issues
LHH’s Federal Funding Set to End in a Month, on November 13
LHH Not Prepared for CMS Re-Inspection as of September 16
LHH Behind Schedule Submitting CMS Re-Enrollment Forms
Health Department is Eliminating Certified Nursing Assistants,
Job Classification, De-Skilling Them to Patient Care Assistants
Update on City Attorney David Chiu’s U.S. DHHS Appeal
by Patrick Monette-Shaw
Laguna Honda Hospital (LHH) was fortunate when the Centers for Medicare and Medicaid Services (CMS) agreed to extend federal reimbursement to cover the costs of care for LHH’s residents through November 13.
We’re now just one month away from when federal funding for LHH is poised to end on November 13. It’s unclear if LHH will seek an extension of the funding from CMS beyond November 13. Mayor London Breed and San Francisco officials have been curiously silent on whether the City will seek an extension beyond November 13 or might step in to pick up the costs of caring for LHH’s remaining 591 residents. And Governor Gavin Newsom’s office has also not indicated whether the State might step in to help with emergency funding.
When State surveyors inspected LHH on October 14, 2021, LHH’s census was 710 residents. At 591 residents still remaining at LHH as of September 26, that means 119 residents have either been discharged, have died, or were transferred to other hospitals for acute care conditions and have not returned to LHH.
Involuntary discharges of residents, most probably to out-of-county facilities, may resume on November 11.
Most worrisome, the July 12 LHH Executive Team presented a report to the LHH-Joint Conference Committee (LHH-JCC) indicating (on page 7) that LHH would submit forms to obtain CMS Re-Enrollment by mid-August to begin the re-certification process, hoping to have CMS conduct an initial facility survey inspection by early September. It appears LHH may be well behind schedule, since it is thought the LHH-JCC has not been updated on whether LHH submitted the re-enrollment forms to CMS in mid-August, and the initial CMS facility survey was not conducted in September. LHH hasn’t indicated just how far behind schedule it is.
Some members of the community are worried about whether City Attorney David Chiu is going along with the shutdown plan for LHH, because of the lack of information on when Chiu’s three appeals — now consolidated into a single docket number case — before U.S. DHHS Administrative Law Judge Steven Kessel will be heard. Chiu faced an October 5 deadline to file prehearing exchanges about his appeals. [More below.]
Only a handful of issues relating to the situation at LHH have recently become available.
Reduction in Costs of External Consultants
The Westside Observer’s September 13 issue reported that three retroactive contracts San Francisco’s Department of Public Health (SFDPH) had issued to assist Laguna Honda Hospital (LHH) prepare for federal and state inspections and apply for Centers for Medicare and Medicaid (CMS) re-certification in order to allow LHH to resume patient admissions and avoid closure might conceivably cost up to $30 million in consultant fees, at $10 million for each contract. The three contracts had been introduced to the Board of Supervisors with terms potentially up to 10 years each.
The Observer is pleased to update readers that the three contracts appear to have been held to slightly over $15 million. On Wednesday, September 21, the Board of Supervisors heard the Tryfacta and Health Services Advisory Group (HSAG) contracts. The Committee adopted recommendations made by its Budget and Legislative Analyst (BLA) that the Committee amend its proposed Resolution by removing the provisions allowing SFDPH to extend the two contracts’ terms to up to 10 years, and/or increase the amount of both contracts to $10 million each. The Committee passed an amendment adopting the BLA’s recommendations, and forwarded a positive recommendation to the full Board of Supervisors to approve the amended Resolution, which will be heard in mid-October.
Given scheduling constraints, the Budget and Finance Committee hasn’t yet heard the third contract — for Health Management Associates (HMA) — by October 7, but by report SFDPH is expected to withdraw its proposal to potentially increase HMA’s contract to $10 million with a 10-year term.
The contracts will reportedly be held to their proposed original amounts, saving the City $15 million. The Tryfacta and HSAG contracts will end in December 2022, while the Health Management Associates (HMA) contract will end on June 30, 2023. It remains unclear why the HMA contract needs to run until June 2023. As we had reported in September, LHH hoped to obtain CMS re-certification by December 2022.
As we also alerted readers in September, it will take ongoing vigilance by community advocates to monitor whether SFDPH will come back again and propose increasing the three contract amounts through additional amendments at a later date.
LHH Unprepared to Pass CMS Re-Certification
From the BLA report issued on September 16, 2022 the Observer first learned LHH was not prepared as of July 19 — months after the three contractors were brought on board — to pass a CMS re-certification survey in November, as initially planned:
“To prepare for recertification with CMS, DPH is undertaking mock surveys to simulate the pending CMS recertification review expected in November 2022. The first mock survey by DPH and Health Management Associates was completed in two phases in June and July 2022 and found that Laguna Honda Hospital would not pass a CMS certification survey.”
The September BLA report provided in a footnote a hyperlink to an 11-page report released by LHH’s acting CEO Roland Pickens dated as far back as July 19 that reported, in part:
“Based on the [first] mock survey results, Laguna Honda would not pass a CMS certification survey if it was conducted today. The mock surveyors cited 39 federal regulations violations, also known as ‘tags’ [F-tags] as part of the statement of deficiencies. These tags reflect deficiencies hospital-wide [sic] and span nearly all disciplines including infection control, resident rights, freedom from abuse, neglect, exploitation; quality of care; and more.”
Why does infection control still remain a huge problem at LHH?
The report prepared by HMA is available here or here (if it is disappeared on-line), and contains nine pages of alarming findings of the on-going problems at LHH, despite the three consultant contracts that began as early as May, if not before.
The mock survey was conducted between June 22 and June 28 to assess LHH’s compliance with CMS’ Conditions of Participation for Skilled Nursing Facilities (SNF’s) and Acute Care hospitals. The mock survey revealed a total of 39 ongoing F-Tag deficiencies that correspond to federal regulations in 13 out of 21 of CMS regulatory groups.
The alarming mock survey findings included:
There were seven additional findings in other categories in the HMA summary of violations of the first mock survey.
Director of Public Health Grant Colfax was scheduled to present an update on the LHH Recertification and Closure Plan to the Health Commission on October 4, 2022, but he gave a scant update mentioning only that he was pleased with progress on the LHH units/neighborhoods in implementing their Quality Assurance and Performance Improvement (QAPI) plans. While that is clearly of interest to CMS for re-certification of LHH, Colfax mentioned nothing else about the many problems LHH is facing to pass re-certification survey inspections, described in more detail below. We’re just a month out from when federal reimbursement is set to in November, and the only thing Colfax could bring himself to comment on was the QAPI initiative.
As part of the plan of corrections following the mock survey, LHH CEO Pickens announced that a Nursing Home Administrator (NHA) position has been added. Pickens failed to mention that the NHA is actually an HSAG employee, who is a temporary authorized through December 31, 2022.
For its part, the July 19 HMA report noted that a Nursing Home Administrator consultant position was added to the HSAG contract to provide expertise to attain compliance with regulations specific to nursing homes. That’s because experienced, licensed Nursing Home Administrators are required to be well versed on CMS regulations SNF’s are required to comply with.
The Westside Observer placed a records request on September 5 to see whether LHH has actually advertised job posting announcements, or had begun to recruit, for a permanent Nursing Home Administrator (NHA) and an Assistant Nursing Home Administrator (AHNA) that Pickens had included on his June 30 LHH major reorganization org chart. SFDPH responded saying it has “no responsive records,” apparently meaning the job postings have not been released and no recruiting efforts to fill the two positions have begun since July.
LHH hasn’t employed a Nursing Home Administrator for the past 18 years, when it replaced Larry Funk with John Kanaley as LHH’s CEO, as reported in July. Had SFDPH realized the value of having LHH run by a NHA deeply experienced with CMS regulatory compliance, LHH might not now be in the mismanagement mess it is has been in for well over a decade.
One observer wondered whether recruiting for the NHA and AHNA positions is being delayed until LHH learns whether it will pass its two CMS recertification inspections, because if it doesn’t pass recertification there might be no need for either of the two positions.
Scope of Services Expanded for HSAG
Neither the initial HSAG contract nor its First Amendment adding $5.2 million to the contract went into much detail about the scope of services to be provided for the now $6,989,564 total contract. The initial HSAG contract was for HSAG to perform survey readiness assessments and mock CMS audit surveys of Laguna Honda Hospital.
Perhaps as a result of the dismal findings from the first mock survey, for the Board of Supervisors Budget and Finance September 21 meeting the BLA revealed more details about the scope of services HSAG is to perform to justify increasing the total contract amount to just under $7 million.
HSAG’s expanded scope of services includes seven areas, including:
Why Is a Budget Wonk an LHH “Incident Commander”?
Baljeet Sangha is the Chief Operating Officer and Deputy Director of the San Francisco Health Network [of community primary care clinics and centers] in the San Francisco Department of Public Health. He was appointed as the Laguna Honda Hospital CMS Recertification Co-Incident Commander. He’s a Manager VIII and earned $289,192 in the Fiscal Year ending June 30, 2022.
The other Co-Incident Commander is Troy Williams, Chief Quality Officer for the San Francisco Department of Public Health’s Community Health Network, and was formerly SFGH’s Director of Quality Management. Williams’ job classification is as a Nursing Supervisor. He earned $326,388 in FY 2021–2022, including $62,582 in “other pay.” Williams, and Maggie Rykowski, SFDPH’s Chief Integrity Officer (whose job classification is also as a Nursing Supervisor) are prominently shown at the top of LHH’s August 2022 organization chart, along with Sangha. In earlier years, SFGH staff were not included on LHH’s org chart. It’s a clear signal that LHH is under the thumbs of this trio of SFDPH managers who have no experience running a skilled nursing facility.
During the September 21 Budget and Finance Committee Hearing on the HSAG Contract, Supervisor Connie Chan asked Mr. Sangha: “What exactly do we expect for results and delivery?”
Sangha’s response to Chan was vague, but he did toss in:
“Those daily ‘roundings’ [across all shifts on the 13 resident neighborhoods] blow up into observations that in any one week can be 6 or 7 thousand observations, which entail [observing] an individual [employee] walking out of [a resident’s] room, have they have performed hand hygiene and are they wearing the correct PPE[Personal Protective Equipment] and then through the whole cycle of the care delivery in the particular area. We are monitoring this and benefiting from the HSAG team coaching just-in-time teach-backs to make sure we effect culture change [of the employees] and partnering with staff and the Labor [Union] partners in those moments. That is really what we are tracking.”
In his reply to Chan’s question about what the City can expect in the way of results on the now almost $7 million contract, Sangha focused on HSAG providing daily roundings to observe whether nursing staff have performed hand hygiene and whether they are wearing the correct PPE, and HSAG providing just in time teach-backs to make effect culture change.
Sangha’s testimony to the Committee was less than reassuring, given the $7 million contract and his salary level as a senior manager. His performance was even less reassuring about his Co-Incident Commander duties at LHH.
To the extent potential closure of LHH and loss of CMS certification is seen as an “incident” needing co-commanders, FEMA defines an incident commander as:
“[An] individual [assigned to be] responsible for all incident activities, including the development of strategies and tactics, and the ordering and release of resources. The Incident Commander has overall authority and responsibility for conducting incident operations and is responsible for the management of all incident operations at the incident site.”
My memory from when I was an LHH employee is that LHH’s CEO retained overall authority for preparing for CMS survey re-inspections when they rarely occurred, although senior nursing management and the Nursing Education Department staff were delegated responsibility for ensuring nursing staff were properly educated and trained on CMS F-Tags and strategies to pass an inspection.
So, why is a SFDPH senior “budget wonk” manager from SFDPH’s Health Network of community primary care clinics who probably has no job experience in a skilled nursing facility environment a Co-Incident Commander of the effort to help LHH regain CMS re-certification — rather than, say, an experienced, licensed Nursing Home Administrator?
This is precisely why LHH has so many problems: SFGH and DPH senior managers having meddled for decades in LHH’s management and operations, with disastrous results!
As a former LHH employee noted in a September 2022 letter-to-the-editor of the Westside Observer:
“The current DPH/LHH leadership can not claim ignorance of SNF standards of care or choose which guidelines they will follow. Their attempt to allocate up to ten million dollars to health care consultants is to redirect attention away from their inadequate administration of San Francisco health care.”
The letter’s author hit the nail on the head as several Westside Observer contributors have noted in many recent articles: LHH’s main problem is that of too much meddling from SFGH and DPH managers who have no experience in skilled nursing facility operations and following CMS’ regulations!
The letter echoed former District 1 Supervisor Sandra Lee Fewer’s observation in the August Richmond Review that “[The problems of substandard care at LHH] clearly could have been prevented and could have been remedied.”
LHH’s August COVID Outbreak and Infection Control Problems
It was somewhat concerning that Sangha alluded on September 21 to potentially continuing problems monitoring staff compliance with COVID-19 infection control precautions, such as hand hygiene and PPE.
After all, when LHH flunked its April 14, 2022 California Department of Public Health (CPDH) inspection survey that led to LHH losing its CMS certification on the same day, of the 22 F-Tag violations on the April survey report one involved F-Tag 880 Infection Control and Prevention. The State inspectors observed 15 nursing staff not following COVID precautions, including 9 Certified Nursing Assistants (CNA’s), 3 Licensed Vocational Nurses (LVN’s), 1 Patient Care Assistant (PCA), and 2 Registered Nurses (RN’s) not following precautions. Inspectors observed the staff not wearing gowns, not wearing N-95 respirators, wearing eye protection on the top of their heads, not wearing face shields, and donning gloves without first performing hand hygiene.
During its September 20 meeting, the Health Commission was presented a report by LHH’s acting-CEO Roland Pickens on behalf of LHH’s Executive Team, that revealed (on page 11) that when it comes to infection control preparedness for a CMS recertification survey, 70% — just 9 — of the facility’s 13 neighborhoods were in survey readiness compliance as of September 16. The other four unit neighborhoods were still not in survey readiness compliance as of September 16. Obviously, that’s not good.
One observer with clinical experience noted:
“If the staff hasn’t been trained and can’t even be educated to pass basic stuff like how and when to wash hands, and don and doff gloves [or gowns] … that is pretty severe mismanagement.”
It’s worrisome that we’ve reached the end of September, and Sangha and his team are still having to do “just-in-time teach-backs” of COVID infection control issues to direct patient care nursing staff.
And it’s troubling — but no great surprise — that the San Francisco Examiner ran an article on September 23, 2022 announcing that LHH had its biggest COVID-19 outbreak in August 2022, reaching 55 COVID-positive patient cases on August 25. LHH has long touted its national reputation in protecting LHH’s residents from COVID infections, and only had six patient deaths between 2020 when the pandemic began and 2021.
Unfortunately, the LHH COVID dashboard the Examiner quoted has had more deaths than the 8 deaths the Examiner had reported. As of October 5 the dashboard now reports LHH had 5 additional patient COVID deaths during 2022, bringing total patient deaths to 11.
Indeed, the dashboard reports show that while LHH had a total of 78 patient COVID cases during 2020 and 2021 combined, LHH has had a total of 211 patient COVID infections during 2022. In addition, while the Examiner didn’t mention it, LHH had a total of 287 COVID infections among staff during 2020 and 2021 combined, but has had a total of 829 COVID infections among staff during the first nine months of 2022. That suggests LHH’s infection control procedures may be lacking.
To be fair, it should be noted visitor COVID restrictions and precautions were relaxed in 2022 to allow for increased visitor access, which may have affected the increase in COVID cases among LHH’s residents and staff. LHH asserts it has increased visitor precautions since the August outbreak by reinstating on-site COVID testing to show negative results before visitors are allowed to enter the facility, and has implemented stricter PPE requirements for LHH staff. Unfortunately, staff non-compliance with infection control measures remains an on-going problem.
The end of the Examiner’s article updated on September 28 quoted Pickens as saying: “At least until November 13 we are fighting one battle, and that battle is recertification.” But to many observers, the biggest battle LHH should be waging is improving the quality of the patient care LHH is mandated to provide, and rapidly improving staff compliance with infection control precautions urgently needed to pass re-inspection surveys.
Since all hospitals and skilled nursing facilities have to report their COVID cases and deaths to the California Department of Public Health (CDPH) which is then transmitted to CMS, CMS and CDPH inspection surveyors must be well aware of LHH’s August COVID outbreak and COVID cases and deaths during 2022 — at the same time that LHH is seeking CMS re-certification and continues to have ongoing infection control prevention deficiencies.
Update of LHH’s Acute Unit
In my September 2022 article, I neglected to include some relevant information concerning Pickens’ assertion LHH had been following the State of California’s Title 22 “Acute Care Hospital” guidelines, rather than focusing on CMS’ regulations governing skilled nursing facilities.
I neglected to note that LHH’s acute medical unit has just five beds. By contrast, LHH has a license for well over 700 skilled nursing facility (SNF) beds, and is considered to be a “distinct part SNF” affiliated with an acute care hospital. The main reason LHH has long held Distinct-Part SNF designation and held on to its five-bed acute unit licensing is because reimbursement to distinct-part SNF’s is significantly higher than reimbursement to free-standing SNF’s not affiliated with an acute care hospital. Historically, LHH’s acute medical unit is rarely used, because residents who need intensive acute care are routinely transferred to actual acute care hospitals for optimal care.
Of note, at some point in 2022 the LHH Executive Team stopped reporting the average daily census of patients in LHH’s acute medical unit to the LHH-JCC Commissioners, lessening transparency of hospital operations. When Pickens raised the ruse that LHH had been following acute care hospital State guidelines rather than federal nursing home regulations, he neglected to say that for a number of years LHH’s acute unit has typically had an average daily census of less than one patient during any given month.
Indeed, meeting minutes of the LHH-JCC’s March 12, 2019 meeting contains testimony from Dr. Derek Kerr that asserted:
“Previously, this Committee addressed the low census on the Acute Rehab Unit, and a Kaizen exercise was organized to boost referrals. Not yet addressed is the very low census on the Acute Medical Unit — just 0.18 patients/day last year.”
The Acute Rehab Unit is for non-LHH patients admitted for intensive physical medicine and physiatry rehabilitation. It is not staffed with acute care nurses, and is not equipped with acute care medical equipment. Patients in the Acute Rehab Unit simply need intensive acute rehabilitation therapy.
By contrast, the Acute Medical Unit is for LHH residents who need short-term acute medical care following medical decompensation who can be cared for in-house for a short period of time rather than being transferred to an acute care hospital having with more advanced medical equipment.
Pickens’ claim LHH had been following acute care hospital guidelines was simply a ruse meant to deflect from LHH’s failure to comply with CMS’ guidelines.
LHH Personnel Staffing
An August 2022 report to the LHH-JCC showed that the vacancy rate of unfilled positions across all of LHH was 12%, which is considered to be relatively high for a City department.
 Behavioral Health/Mental Health Staff
Behavioral Health/Mental Health Staff
Given LHH’s high percentage of behaviorally challenged residents, the 48.8% vacancy rate among behavioral health staff at LHH is very concerning.
Of 1.0 budgeted FTE Psychiatric technicians, the single position is vacant, for a 100% vacancy rate. However, Pickens June 3 Pilot Org chart said there would be two psych tech positions. Does that mean that of both psych tech positions are vacant? Of 2.0 budgeted FTE Clinical Psychologists, both positions are vacant, also for a 100% vacancy rate.
Of 2.0 budgeted FTE Psychiatric Social Workers, one of the positions is vacant, for a 50% vacancy rate. Of 5.0 budgeted FTE Senior Psychiatric Physician Specialists, 2.2 FTE positions are vacant, for a 42.7 vacancy rate. Not having enough psych MD’s and Clinical Psychologists is worrisome!
How can LHH be providing an appropriate level of care for these residents safely with an almost 50% vacancy rate?
 Nursing Staff
Nursing Staff
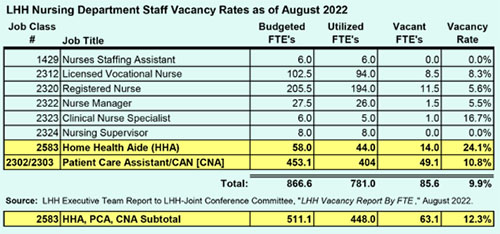
The August 2022 vacancies report to the LHH-JCC showed that the vacancy rate of unfilled positions across the eight job classification codes in LHH’s Nursing department is just under 10%, which suggests the quality of care being provided to LHH’s residents may be suffering, with overworked staff.
Of note, the vacancy rate for nursing staff in the Certified Nursing Assistant (CNA), Patient Care Assistant (PCA), and Home Health Aide (HHA) job classifications stood at a combined 12.3% vacancy rate with a combined vacancy of 63 positions. This doesn’t bode well for passing a CMS reinspection survey.
There are some important differences in the job duties between the three job classifications. The main differences between them involve levels of education, license obtained, and salary levels.
CNA’s are often responsible for setting up medical equipment such as IV drips and oxygen supplies, measuring vital signs, and observing changes in the patient’s condition, in addition to services provided by a PCA or HHA. CNA’s receive extensive training and certification from an authorized program, undergo supervised clinical experience, and passing the equivalent of a state license (certification) examination.
PCA’s — a.k.a., Personal Care Aides — typically assist with personal-care issues, including bathing, toileting, dressing, and grooming. HHA’s receive training, usually from a vocational school or community college, and then must also pass a state certification exam. They help with dressing, toileting, and checking vital signs. HHA’s can also assist with braces, artificial limbs, and caring for patients’ skin. Administration of medication is typically restricted to Licensed Vocational Nurses and Registered Nurses.
Mr. Pickens’ Executive Team Report for the August 9 LHH-JCC meeting reported on slide 20 that “40 patient care assistants would be on-boarded on September.” In response to a records request, SFDPH indicated that “offers were made to over 40 candidates, of which 28 accepted and either already started in September or will start in October.” That suggests that only 70% of the 40 anticipated new hires were “on-boarded,” but SFDPH neglected to indicate how far into October some of the new hires will be brought on board. Alternatively, the 28 new PCA’s represent just 44.4% of the 63 combined vacancies between CNA’s, PCA’s, and HHA’s. Again, this doesn’t bode well for passing a CMS reinspection survey, either, given the time it will take to train them on LHH’s operations and the overall staffing shortage.
LHH has “deskilled” many CNA positions to PCA’s and HHA’s as a budget-cutting measure. De-skilling refers to changing the way a job is done so less skill is needed to do it, skilled labor is diminished, special skills to do the work is removed, and organizations can save money by paying workers less.
Average annual total pay throughout SFDPH (not just at LHH) for a 2,080 hour-per year (full-time position) in the fiscal year ending June 30, 2022 for a CNA was $100,719 — compared to $81,063 for a PCA, and $76,701 for an HHA, all excluding fringe benefits. Deskilling the CNA positions saves the Department of Public Health a significant amount of money.
In the six years between FY 2015–2016 and FY 2021—2022, across SFDPH (including both SFGH, LHH, and its San Francisco Health Network clinics), the number of CNA positions has dropped by 45 (from 131 to 86) at the same time PCA positions increased by 22 (from 545 to 567).
A response to another public records request revealed that throughout SFDPH’s various divisions — SFGH, LHH, and its community primary care health facilities — the Department is eliminating CNA positions and converting those positions to lower-paid Patient Care Assistants through attrition.
You have to wonder why the CNA’s have allowed their union, SEIU Local 1021, to agree to the deskilling and elimination of their job classification code and jobs. After all, Local 1021’s current president is Theresa Rutherford, who began her employment with San Francisco’s Department of Public Health as a CNA working at LHH. Now that Rutherford is collecting an inflated salary working full-time for the Union, does she no longer care for the plight of her former LHH CNA co-workers?
 Nutrition Services Staff
Nutrition Services Staff
Of the 22 F-Tag deficiencies across the nine different Regulatory Groups of CMS violations during LHH’s State survey between October 14, 2021 and April 13, 2022 that resulted in CMS de-certifying LHH, none of the deficiencies involved the Food and Nutrition Services regulatory group governed by Federal Code of Regulations §483.60. In other words, LHH’s Nutrition Services Department had not been found to have violated any of CMS’ F-Tags.
However, the HMA report following LHH’s first mock survey in late June noted severe problems with the Nutrition Services Department involving menus, food, and snacks at bedtime, noted above.
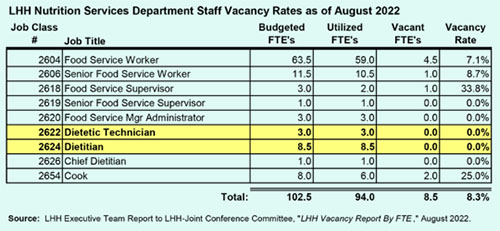
With that said, it’s very curious why the as-needed staffing contract with Tryfacta stated an immediate need to hire seven full-time equivalent (FTE) dieticians and two Dietetic Technician’s FTE’s on a temporary basis, between June 17 and December 17, 2022 — although if LHH has not yet regained CMS certification by December 17, we may see Tryfacta’s contract extended for a longer period of time.
Indeed, as the table included here shows, the Dietician and Dietetic Technician positions currently have no staffing vacancies. So, it’s not known why LHH’s Nutrition Services Department needed to be staffed up with a total of nine additional FTE positions.
There are three issues regarding Nutrition Services and LHH’s kitchen, which appear to be separate issues potentially unrelated to the CMS re-inspection survey.
First, the need to replace LHH’s kitchen floor has been presented to the three JCC Health Commissioners during LHH-JCC meetings. By report, when the replacement hospital was opened in 2010, the kitchen floor contained embedded glass, which broke due to heavy kitchen equipment and carts being used. That led to severe water damage in the kitchen, which then led to mold problems. No information has been provided about the project timeline or whether the project has been completed. A records request was placed to find out the budgeted dollar amount to replace LHH’s kitchen floor and the project timeline.
Second, by report the freezers in LHH’s kitchen have been broken down for months and LHH reportedly had to rent freezer truck(s) parked in LHH’s parking lot. Another records request was placed to find out whether the freezers have been replaced yet, and the dollar amount to replace the freezers.
Third, during the LHH kitchen floor replacement project a vendor will presumably be required to provide food and meal delivery to LHH’s residents that meets State standards, including menus that address appropriate diets, texture modifications, variety, and cultural and resident preferences. Another records request was placed to find out whether an RFQ or RFP has been issued seeking qualified vendors to provide food and meal delivery to LHH’s residents during the LHH kitchen floor replacement project, and whether a vendor been selected.
SFDPH responded to the three records requests by invoking a 10-day extension allowed by the Sunshine Ordinance, and said responses to the three records requests will be provided by October 13, 2022.
Status of City Attorney’s Appeals to U.S. DHHS
There are concerns in the community that Mayor London Breed and those who serve her are posturing about rescuing Laguna Honda Hospital and may not be doing enough.
As I wrote in the end of July (“City’s Pathetic Defense of LHH”), City Attorney David Chiu had filed three appeals with the U.S. Department of Health and Human Services (DHHS) on February 15, April 25, and May 28, challenging findings by California Department of Public Health surveys and CMS’ decision to terminate LHH’s participation in CMS’ provider reimbursement program.
On June 2, 2022 DHHS Administrative Law Judge (ALJ) Steven Kessel issued an order consolidating Chiu’s three appeals into a single docket number (C-22-555). Kessel set an August 31 deadline for CMS and an October 5 deadline for City Attorney Chiu to submit any “prehearing exchanges.”
According to DHHS’ Department Appeal Board web site, unless an Administrative Law Judge directs otherwise, a prehearing exchange (or here) includes: lists of proposed exhibits and proposed witnesses;copies of proposed documentary exhibits; written statements (sworn affidavits or statements made under penalty of perjury) of all proposed witnesses offered in lieu of direct testimony; any prior statements of proposed witnesses other than those offered by proposed witnesses that relate to issues which might be raised at hearing; and a prehearing brief that provides a party’s written arguments about all matters of law and fact(s) at issue in the case.
Presumably, LHH’s October deadline was set so that our City Attorney could potentially raise any objections to materials and issues CMS may have chosen to submit to Kessel.
Other rules for prehearing submission requirements include: The ALJ may order other prehearing submissions in addition to those stated above; in complex cases, the ALJ may order two exchanges of proposed exhibits and lists of exhibits and witnesses; each party must file all of its prehearing submissions at one time even if it files the submissions prior to the deadline the ALJ established, and may not file its submissions piecemeal; untimely submissions are prohibited; and a party may not call a witness at an oral hearing who was not listed on that party’s witness list or offer an exhibit not listed or timely furnished to the opposing party.
On October 5, the Westswide Observer submitted a records request to the City Attorney Chiu’s office requesting the entire packet of prehearing exchanges Chiu filed with Judge Kessel. The City Attorney’s office responded to our immediate disclosure records request providing Chiu’s prehearing exchanges on an expedited basis on the same day.
The single PDF file provided by Chiu’s office is a 4,891-page document, and is 357 megabytes in file size. The Observer extracted Chiu’s Prehearing Exchange Brief to Administrative Law Judge Steven Kessel, and also extracted Chiu’s Witness and Exhibit lists.
In the Introduction section of Chiu’s Prehearing Exchange Brief (starting on page 6) he asserts that the California Department of Public Health (CDPH), “erroneously assessed a violation of 42 C.F.R. Section 483.25(d) based on the mere presence of illicit drugs and contraband in the facility.”
§483.25 of the Code of Federal Regulations governs “Quality of Care.” There are 17 F-Tags covered under this section and all of them constitute sub-standard quality of care. Chiu’s initial Appeal filed on February 15, 2022 and two additional appeals focused heavily on asserting CDPH had wrongly found violations around incidents involving F-Tag 689, “Free of Accident Hazards/Supervision/Devices.” Chiu’s three appeals filed with the U.S. DHHS Appeals Board have respectfully disagreed that any of the illicit drugs and contraband found with LHH residents cited as incidents were “accidents” or “hazards” under F-Tag 689.
Chiu’s 30-page Brief asserts CDPH applied a strict liability standard against LHH, in error.
As a quick summary, the Introduction to his Brief states “Laguna Honda requests the court overrule CMS’s remedies and its decision to terminate Laguna Honda’s Medicare provider agreement. Laguna Honda also requests that the court find that CMS erred when denying payments for new admissions, and when assessing the civil monetary penalties associated with Section 483.25(d).”
According to DHHS’ Department Appeal Board a hearing date before Judge Kessel has not been set yet. Watch this space.
As strong as Chiu’s Brief appears to be at having a shot of prevailing on its merits, having seen a few of Judge Kessel’s rulings in a handful of other cases there are concerns Chiu’s Prehearing Brief and three Appeals may not convince Kessel.
Monette-Shaw is a columnist for San Francisco’s Westside Observer newspaper, and a retired City employee. He received a James Madison Freedom of Information Award in the “Advocacy” category from the Society of Professional Journalists–Northern California Chapter in 2012. He’s a member of the California First Amendment Coalition (FAC) and the ACLU. Contact him at monette-shaw@westsideobserver.com.